|
|
|
Free Neuropathology 6:10 (2025) |
|
Review |
|
Neurooncology: 2025 update |
|
Michel Mittelbronn1,2 |
|
|
Corresponding author: |
|
Submitted: 23 February 2025 |
|
Keywords: Neurooncology, Neuropathology, Brain tumors, Glioblastoma, Brain metastasis |
|
Abstract This collection of studies highlights groundbreaking advancements in brain tumor research, particularly primary CNS tumors and brain metastasis. One major focus is the tumor microenvironment, where alterations in cerebral microcirculation and hypoxic-ischemic conditions have been shown to influence metastatic progression. In glioblastoma, recurrent tumors exhibit distinct DNA methylation profiles, and global DNA methylation has emerged as an independent diagnostic marker for IDH-wildtype glioblastoma. A whole-tumor perspective further emphasizes the extensive intratumoral heterogeneity driving glioblastoma evolution. The immune landscape of glioblastoma is another key area of research. Cranioencephalic functional lymphoid units have been implicated in tumor progression, while time-dependent single-cell phenotyping offers novel insights into immune cell dynamics within glioblastoma. Additionally, histone serotonylation has been identified as a critical epigenetic regulator in ependymoma tumorigenesis. Diagnostic and prognostic innovations are paving the way for improved patient care. Histomorphological features provide enhanced prognosis prediction for glioblastoma patients. Confocal laser microscopy enables real-time intraoperative histopathological diagnostics, and sequencing of cerebrospinal fluid-derived cell-free DNA presents a promising non-invasive diagnostic approach. Together, these top studies of 2024 underscore the complexity of brain tumor biology and the integration of epigenetics, immune interactions, and advanced diagnostics into clinical practice. These insights mark significant progress toward personalized treatment strategies and improved outcomes in neurooncology. |
|
Introduction Artificial intelligence is currently a hot topic and is intended to make work easier for humans. However, there are still numerous challenges in academic literature research, particularly due to hallucinations that lead to the generation of inconsistent or completely incorrect references [Albuck et al., 2024]. Nevertheless, the author of the current article wanted to give it a try to see whether his work could be simplified through the use of artificial intelligence, or more specifically, large language models (LLMs), or at least gain some additional inspiration about interesting primary research articles in the field of neurooncology published in 2024. Therefore, the following very generic question was posed to three LLMs (https://chatgpt.com/; https://gemini.google.com/app and https://www.perplexity.ai/): ‘Could you please provide me with the 10 most influential primary research papers published in neurooncology with a link to neuropathology in the year 2024?’. ChatGPT proposed several non-existent articles, including a review article supposedly authored by the writer of the present review. However, it altered the author list as follows: 'Neurooncology: 2023 Update'; Authors: Wisoff JH, Sanford RA, Heier LA, et al. Published in: Free Neuropathology, 2023 [Mittelbronn, 2023]. In addition, 5 of the 10 proposed 'primary research papers' were actually podcasts. By rephrasing and adjusting the prompt, some improvements and corrections were achieved; however, the results improved only partially and gradually. PERPLEXITY suggested exactly the 10 papers from the Top 10 Series in Neurooncology published in Free Neuropathology last year but re-dated all articles from 2023 to 2024 [Mittelbronn, 2024]. After being re-prompted, PERPLEXITY explained that it would be inappropriate to speculate or provide inaccurate information about influential papers from 2024. Only GEMINI – both initially and after several attempts or re-prompting – refused to provide some suggestions of real scientific papers, instead recommending journals, search engines such as PubMed (https://pubmed.ncbi.nlm.nih.gov/) or Google Scholar (https://scholar.google.com/). As a result, unfortunately, not a single of the different LLMs was useful for the compilation of influential primary scientific papers in the field of neurooncology of this year’s edition. Therefore, the author returned to a more traditional approach, screening thousands of titles and abstracts related to key search terms in the field (e.g., brain tumor, glioma, meningioma, brain metastasis, neurooncology, etc.). In contrast to last year, however, fewer novel treatment approaches in neurooncology were identified. Of note, with 29 retractions of papers related to the keyword 'glioblastoma' in 2024 (compared to 22 in 2023 and 9 in 2022, and similarly high number of publications), along with multiple corrections, a worrisome increase in potentially sloppy scientific behavior in this field was observed. Nevertheless, numerous excellent primary research articles were identified and subjective selection was a challenge. As usual, the goal was to provide a collection of articles ranging from basic research findings to novel diagnostic or prognostic criteria, technical and methodological innovations, and therapeutic approaches. With this, the “top ten” series in neurooncology for 2024 reads as follows:
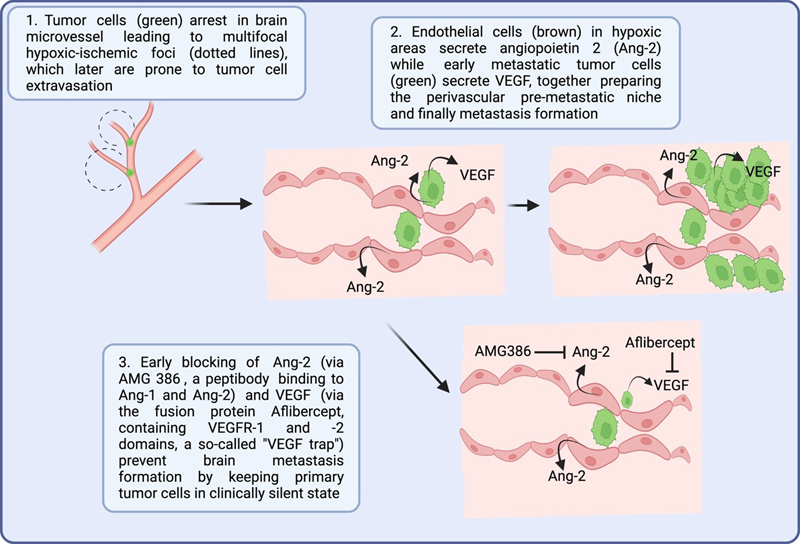
1. Impact of disturbed cerebral microcirculation and hypoxic-ischemic microenvironment on brain metastasis development [Roesler et al., 2024] Although the basic steps of brain metastasis formation, including – amongst others – detachment of cancer cells from the primary tumor and intravasation into the blood stream, followed by adhesion to brain endothelial cells and finally extravasation into as well as colonization of the brain is reiterated, the exact mechanisms and time-dependent sequences are not fully understood. In a previous groundbreaking work of Kienast et al., the metastatic ways of individual cancer cells could be traced over several months in a murine model with real-time multiphoton laser scanning microscopy [Kienast et al., 2010]. With this, the authors could identify the initial arrest of cancer cells at cerebral blood vessel branches followed by angiogenic processes or vessel cooption after early extravasation. Using a similar methodological approach, Roesler et al. were now able to show a similar intravascular tumor cell arrest in brain microvessels before extravasation and formation of micrometastases [Roesler et al., 2024]. Of note, as a most novel finding, already 24h after intracardiac injection of tumor cells, prominent hypoxic-ischemic tissue alterations were observed in the brain that were partly well corresponding with areas, in which metastasis formation was detected at a later timepoint. In the hypoxic-ischemic areas, an upregulation of Ang-2, MMP9 and VEGF was observed in brain endothelial cells leading to the hypothesis that those hypoxia-associated molecules might be at least partly responsible for the seeding of metastatic cells in the brain. To corroborate this hypothesis, the authors also used a transgenic, endothelial-specific Ang-2 gain-of-function approach that revealed an increase of numbers and volumes of brain metastases compared to wild-type animals thereby indicating that extravasation of cancer cells into the brain parenchyma is Ang-2 dependent. The findings of the study were in line with previous findings showing that Ang-2 expression correlated with BBB disruption, impaired tight junctions and increased blood vessel permeability in a murine triple-negative breast cancer model [Avraham et al., 2014]. The findings of Roesler et al. indicate that Ang-2 and VEGF are crucial for the formation of brain metastases via shaping a tumor-supporting pre-metastatic niche, therefore being potential treatment targets, especially in an early phase. With a novel, early pre-metastatic inhibition of Ang-2 (via the AMG 386 peptibody) and/or VEGF (via aflibercept, a fusion protein with VEGFR1 and VEGFR2 domains serving as a so-called “VEGF trap”), the metastatic cerebral tumor cell load could be considerably reduced (see Figure 1). Similar findings were obtained in other previous murine brain metastasis models in which a combined inhibition of Ang-2 and VEGF reduced the number and volume of brain metastases while extracranial metastases did not show a positive treatment response [Bohn et al., 2017; Kovalchuk et al., 2020]. In summary, Roesler et al. present a novel mechanism for brain metastatic processes linked to an increase of Ang-2 and VEGF in the cerebral pre-metastatic niche which are induced by focal hypoxic-ischemic events most probably caused by occlusion of brain capillaries by tumor cells. Showing a significantly reduced cerebral tumor cell load by early dual inhibition of Ang-2 and VEGF, this treatment approach could be highly promising as a prevention strategy in patients suffering from highly malignant tumors with a high risk to develop cerebral metastases. Figure 1: Concept of brain metastasis formation and therapeutic prevention
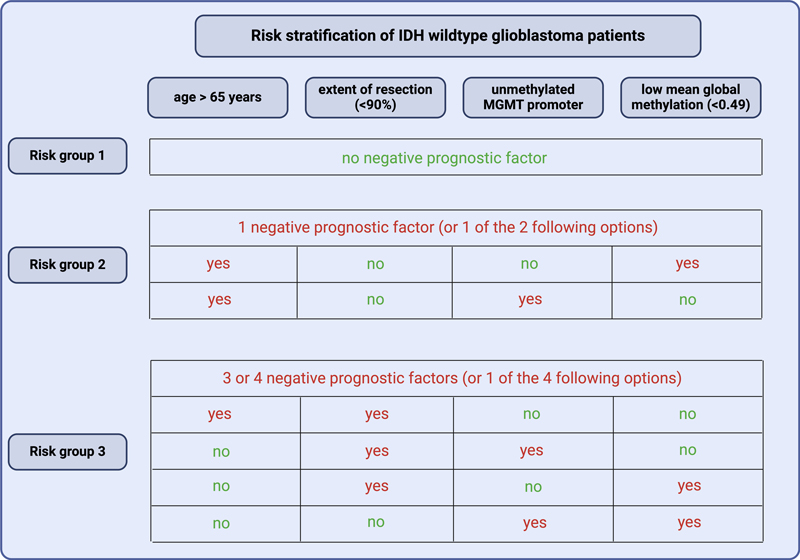
2. Global DNA methylation as independent diagnostic marker in IDH-wildtype glioblastoma [Eckhardt et al., 2024] Large population-based studies still report median survival times of slightly more than 6 months for glioblastoma patients that could be considerably increased to a median of 14.8 months in cases with maximum treatment including neurosurgical resection followed by radiochemotherapy [Brodbelt et al., 2015]. Of note, approximately 30 % of all glioblastoma patients survive 2 years or longer after initial diagnosis. Apart from age, MGMT promoter methylation, extent of resection and follow-up treatment, there is not much known about glioblastoma-intrinsic tumor biological factors that might well predict patient prognosis. Nowadays, neuropathological diagnostics in the field of neurooncology is most precisely performed by DNA methylation profiling [Capper et al., 2018]. Within the class of IDH wildtype glioblastoma, mainly 3 subclasses could be defined: receptor tyrosine kinase I (RTK I), RTK II and mesenchymal subclass, however without showing any relevant survival differences [Drexler et al., 2023b]. In general, only poor data is available about the potential prognostic impact of methylation differences within distinct tumor entities. To address this question, Eckhardt et al. assessed 492 primary and 31 relapse IDH wildtype glioblastomas that all received similar standard treatment regimen. Although no unequivocally clear methylation signature associated with patient survival could be detected, the median methylation rate of 0.49 significantly split the cohort in long (median methylation above 0.49; median overall survival of 18 months) and short (median methylation level equal or below 0.49; median survival of 13 months) time survivors. The optimal cut-off level was determined as a beta value of 0.458 that allowed for identifying a smaller subgroup of 73 patients with a median overall survival of only 9.2 months. Of note, the mean methylation level was an independent prognostic marker in a multivariate analysis together patient age, MGMT promoter methylation status and extent of resection, all factors that are known as prognosticators for a long time. The authors further showed that RTK I subclass glioblastoma had the worst median survival reaching 14.2 months while displaying significantly lower mean methylation levels compared to its counterparts that reached 15 months (RTK II) and 18.8 months (mesenchymal). However, the mean methylation levels were still significantly associated in RTK I and II subclasses. Combined risk classes including mean methylation level, age, extent of resection and MGMT promoter methylation could further increase the prognostic prediction by splitting the cohort into a risk factor-free subgroup reaching 39 months of median survival while the worst subgroup only reached 8.3 months (Figure 2). While immune cell infiltration could be bioinformatically ruled out as underlying explanatory factor, higher mean methylation levels were associated with better radiosensitivity, therefore at least providing a hypothesis why the patient subgroup with high beta values survived longer. These findings were also corroborated in a glioma cell line panel exhibiting better radiosensitivity in cells with a higher beta value. In summary, the authors provide a novel, highly important risk stratification for IDH wildtype glioblastoma patients that might also pave the way for new treatment stratifications in the future. However, a comparison with other tumor entities could not confirm high methylation levels as being associated with tumor aggressiveness in general. Figure 2: Risk stratification for IDH wildtype glioblastoma patients.
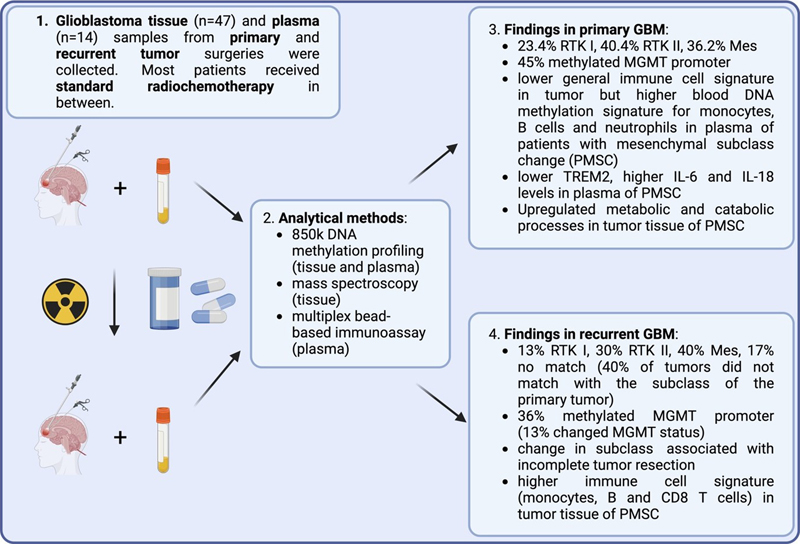
Patient age over 65 years, extent of less than 90 % of the contrast-enhancing tumor area, an unmethylated MGMT promoter and a low mean global methylation beta value of less than 0.49 are considered as negative prognostic factors. Median overall survival times are as follows: risk group 1: 39 months; risk group 2: 19 months; risk group 3: 8.3 months. 3. Change in DNA methylation profile in recurrent glioblastoma [Drexler et al., 2024] DNA methylation profiling has become a highly reliable and unbiased reproducible diagnostic tool in neuropathological routine diagnostics [Capper et al., 2018]. However, only poor data exist about a temporal change of DNA methylation upon treatment in malignant brain tumors that might have an impact on treatment resistance. To address this question, Drexler et al. assessed paired primary and recurrent glioblastomas of 47 patients by DNA methylation from tumor bulk and plasma, mass spectrometry and multiplex bead-based immunoassay [Drexler et al., 2024]. A potential change even in glioblastoma subclasses might be of importance as previous analyses revealed that mesenchymal, RTK I and RTK II subclasses differed in patient survival with 15.5 months, 16 months and 27 months, respectively [Dejaegher et al., 2021]. In the primary glioblastoma cohort of Drexler et al., DNA methylation profiling revealed the following subclass distribution: 23.4 % RTK I, 40.4 % RTK II and 36.2 % mesenchymal while this composition changed to 12.8 % RTK I, 29.8 % RTK II, 40.4 % mesenchymal and 17 % with no match with a known class (Figure 3). In total, 40 % of all recurrent GBM did not match with the subclass obtained in the primary tumors (including 17 % of cases with no match). The highest percentage of transitions was towards the mesenchymal subclass (72.7 %). Thirteen percent of all patients showed a switch of the MGMT promoter methylation status, mostly from a methylated to a non-methylated status, a finding that is in line with previous analyses performed in primary and recurrent glioblastoma [Choi et al., 2021]. The authors also analyzed multiple clinical-pathological parameters but mostly found incomplete resection of contrast-enhancing tumor parts as a significant factor for subclass transition in the recurrent situation. While the cellular composition did not considerably vary between the groups with and without subclass change in general, the cohort undergoing a switch towards a mesenchymal phenotype showed for example a decreased number of immune cells in the primary tumor tissue, however did not reach the level of significance when the analyses were repeated for immune cell subtypes. In contrast, higher methylation signatures were observed for monocytes, B cells and neutrophils in blood of patients in the primary situation later showing a subclass switch towards a mesenchymal phenotype compared to the cohort with stable glioblastoma subclass in the recurrent situation. Proteomic analysis revealed a stronger metabolic and catabolic processes in the primary tumor tissue of patients later undergoing a switch to mesenchymal subclass. Of note, no association of subclass changes with patient survival was observed. This study is of high importance for the understanding of temporal molecular changes in glioblastoma and underscores the necessity to re-perform full molecular assessment in the recurrent situation, especially as also broadly accepted molecular biomarkers such as MGMT promoter methylation status may change over time. To which degree radiochemotherapy induces the temporal switch towards a mesenchymal subclass phenotype has to be further elucidated. Figure 3: Temporal molecular change between primary and recurrent glioblastoma
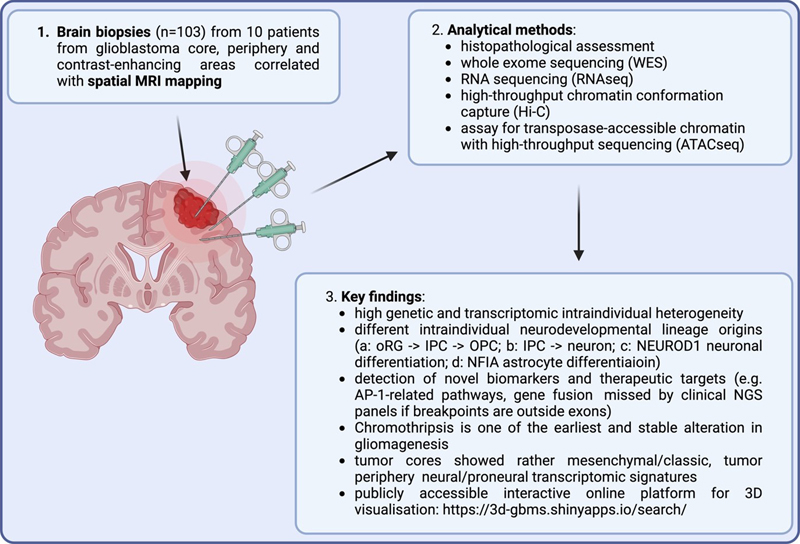
4. Glioblastoma evolution and heterogeneity from a whole tumor perspective [Mathur et al., 2024] Glioblastoma is a highly heterogenous neoplasm composed of both tumor and non-neoplastic cells of the microenvironment. In addition, little is known about the overall molecular heterogeneity including genetic, epigenetic and/or metabolic features as diagnostics is mostly performed on smaller bulk tissue parts. In a previous large-scale approach, a glioblastoma atlas linking classical histomorphological features with transcriptional profiles, the latter assessed by in-situ hybridization, revealed a strong regional molecular heterogeneity partly related to microscopic characteristics [Puchalski et al., 2018]. However, as these previous findings were also derived from preselected tissue blocks not representing the entire regional spectrum of glioblastoma, Mathur et al. sampled multiple tissues (n = 103) from the 10 patients using 3D surgical neuronavigation to obtain representative areas of the tumor core, periphery and contrast-enhancing regions [Mathur et al., 2024]. Furthermore, the biopsy positions were correlated with preoperative MRI scans to generate a representative 3D model of the entire glioblastoma. The small biopsy samples were assessed by histopathological analyses, high-throughput chromosome conformation capture (Hi-C), whole exome sequencing (WES), RNA sequencing (RNA-seq) as well as assay for transposase-accessible chromatin with high-throughput sequencing (ATAC-seq, for tissue and single nucleus) (for summary, see Figure 4). The authors detected a vast genetic and transcriptional heterogeneity within the patients. Only one out of the ten patients showed a consistent signature in all biopsies regarding the previously published, gene expression-based molecular classification into proneural, neural, classic or mesenchymal subtypes while all other patients displayed mixed intraindividual signatures [Verhaak et al., 2010]. Of note, tumor biopsies from the tumor cores more frequently showed a mesenchymal or classic signature while more peripheral biopsies revealed rather neural or proneural signatures. The authors also discovered distinct neurodevelopmental transcriptomic signatures such as for example glioblastoma with a gain of chromosome 7 (with the EGFR, PTPRZ1 and PTN genes) being associated with glioblastoma cells in an intermediate progenitor cell (IPC) transit-amplifying state or – in contrast - glioblastoma with a primitive neuronal component, however without a gain of chromosome 7, showing transcriptional signatures typically observed in cells differentiating from IPCs to neurons. Additional signatures in the tumor center comprised an immune-hot microenvironment with interferon signaling and T cell infiltration versus immune-cold areas with a mesenchymal transcriptomic signature. While most mutations were highly heterogenous, chromothripsis seems to be a very early event in gliomagenesis with virtually no intraindividual heterogeneity. Most importantly, the authors presented several novel potential diagnostic biomarkers and treatment targets, such as the activator protein 1 (AP-1) pathway or several gene fusions that were missed by clinical NGS analyses as breakpoints were outside exons. With this work, Mathur et al. considerably contributed to the understanding of glioblastoma evolution and heterogeneity and provide promising therapeutic targets for further assessment. For more in-depth exploration of the findings, a publicly accessible interactive online platform is available: https://3d-gbms.shinyapps.io/search/. Figure 4: 3D glioblastoma evolution and heterogeneity: methodological approach and key findings.
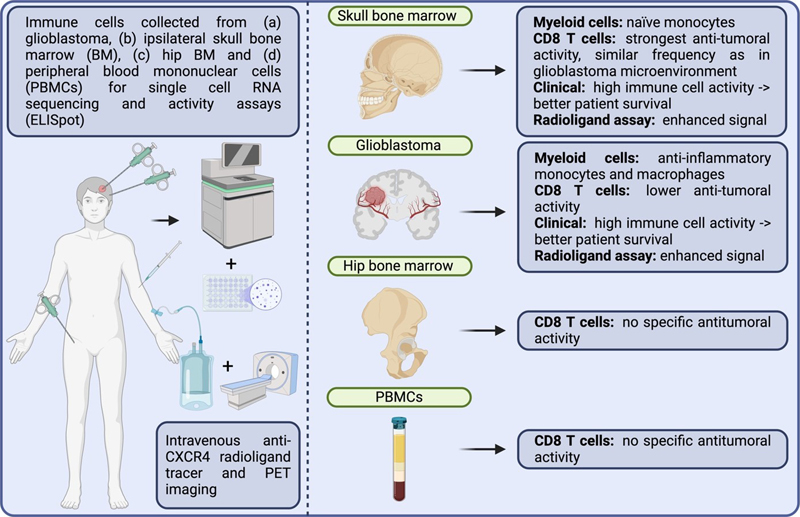
Abbreviations: oRG: outer radial glia; IPC: intermediate progenitor cell; OPC: oligodendrocyte precursor cell; NEUROD1: neuronal differentiation 1 (transcription factor); AP-1: activator protein 1 (transcription factor). 5. Cranioencephalic functional lymphoid units in glioblastoma [Dobersalske et al., 2024] Bridging veins allow for an immunological communication between CNS and skull bone marrow crossing the arachnoid barrier by connecting CNS blood vessels with the meningeal blood circulation and finally the sinusoidal vasculature of the bone marrow [Smyth et al., 2024]. As hematopoietic stem and progenitor cells are located in the skull bone marrow, however not well studied in the context of human diseases, Dobersalske et al. intended to assess the immune cell properties in those areas in regional proximity to human glioblastoma, a condition known for its highly immunosuppressive nature [Dobersalske et al., 2024]. Using a CXCL12 analog radioligand tracer for CXCR4, a marker for hematopoietic and immune cells, the authors found surprisingly high activity in the ipsilateral skull bone marrow and meninges related to the glioblastoma localization in usually older glioblastoma patients. In a single-cell RNA sequencing approach from corresponding (a) glioblastoma samples, (b) ipsilateral bone marrow of the skull, (c) peripheral blood mononuclear cells (PBMCs) and (d) distal hip bone marrow, considerable differences in immune cell compositions were found. Regarding the myeloid cell compartment, mostly naïve monocytes were found the ipsilateral skull bone marrow contrasting anti-inflammatory monocytes and macrophages, predominantly found within glioblastoma. Of note, a strong accumulation of effector-type, glioma-reactive CD8+ T cell activity was detected in the skull of ipsilateral bone marrow whereas a lower activity was found in intratumor CD8+ T cells. Both CD8+ T cells from PBMCs and ipsilateral bone marrow were able to experimentally reproduce memory and effector T cells, while intratumor T cells failed. Of note, the antitumoral activity of skull bone marrow derived CD8+ T cells was higher compared to counterparts derived from PBMCs, distal hip bone marrow or the glioblastoma microenvironment. Similarly high frequencies of tumor-reactive T cells were found in skull bone marrow compared to the intratumor microenvironment, indicating an immune cell trafficking between both compartments. Using the aforementioned radioligand tracer, a significantly longer survival benefit for glioblastoma patients with stronger intratumor and skull bone marrow immune cell activity was observed already in a relatively small patient cohort (n = 52). Taking the clinical impact into account, these findings imply that the skull bone marrow immune cell niches should be absolutely protected during neurosurgical and subsequent radiotherapeutic intervention. In summary, Dobersalske et al. shed a new light of the local antitumoral immune cell activities in glioblastoma patients that needs to be considered for future immunotherapies (for summary, see Figure 5). Figure 5: Cranioencephalic functional lymphoid units in glioblastoma.
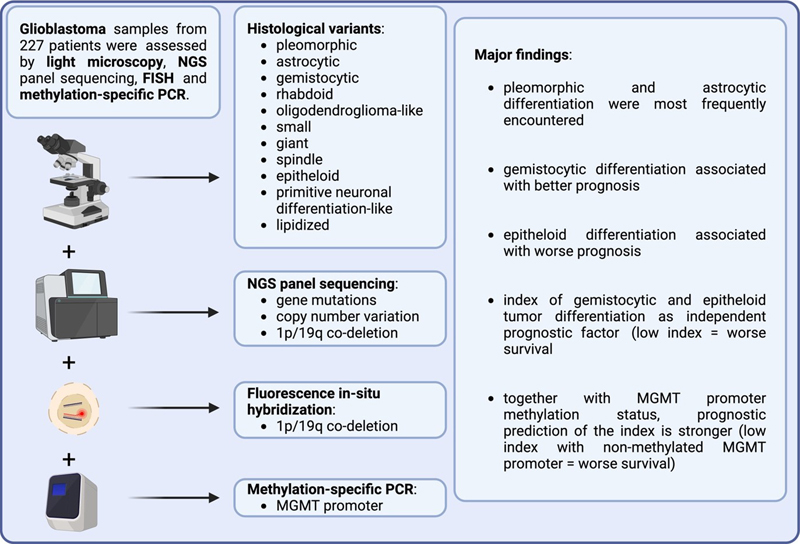
Left side: methodological set-up. Right side: major findings according to compartment. 6. Prognosis prediction via histomorphological features in glioblastoma [Kirishima et al., 2024] Neuropathological tumor diagnostics is more and more shifting away from the previous gold standard of microscopic analysis to more unbiased molecular methods mostly including genetic and epigenetic assessment for both diagnostic precision as well as prediction for treatment response and patient survival. As molecular, especially epigenetic features seem to be more stable than the highly variable morphological features in glioblastoma, it is extremely important to always sample enough tissue from all different tumor areas (e.g. core, periphery, contrast-enhancing areas, necroses etc.) [Mikkelsen et al., 2021]. It is very interesting for neuropathologists if complex histomorphological assessments can still compete with modern molecular diagnostics. Kirishima et al. undertake the endeavor to explore if distinct morphological features may still be of prognostic value in glioblastoma. As for today, a few studies showed worst survival for some glioblastoma subtypes such as epithelioid or rhabdoid variants, no unequivocally clear association of any specific morphological phenotype with clinical prognosis could be detected [Mallick et al., 2022]. Furthermore, most classical microscopic characteristics necessary for the diagnosis of glioblastoma, such as pseudopalisading necrosis or microvascular proliferations, are no longer sufficient for this diagnosis as they might also be found in IDH-mutant astrocytoma [WHO classification of brain tumors, 2021]. Therefore, the authors of the present study analyze 227 primary glioblastoma according to the WHO criteria for the classification of tumours of the central nervous system from 2021 and additionally assessed the following microscopic features in 10 % increments: pleomorphic, astrocytic, gemistocytic, rhabdoid, oligodendroglioma(ODG)-like, small, giant, spindle, epithelioid, primitive neuronal differentiation(PND)-like and lipidized [Kirishima et al., 2024; WHO classification of brain tumors, 2021]. For histomorphological assessment to construct a survival prediction model, the largest, most representative areas were analyzed by two board-certified pathologists. Of note, also NGS panel analysis for genomic profiling, including assessment of gene mutations, copy number variation and 1p/19q co-deletion as well as methylation-specific PCR to determine MGMT promoter methylation status were performed leading to an integrated final diagnosis together with histological and immunohistochemical (e.g. for IDH1-R132H) features. As major morphological variants, pleomorphic (33 % of total tumor area) and astrocytic (29.1 %) differentiation were reported. Most interestingly, if glioblastoma showed epithelioid tumor cells in more than 30 % of total tumor cells, patients displayed an unfavorable prognosis independent of clinical parameters, treatment or molecular alterations. The most favorable prognostic values for glioblastoma patients could be achieved by calculating a combined score taking into account both gemistocytic and epithelioid areas as follows: % area of gemistocytic cells minus 4 x % area of epithelioid cells. A value of less than 20 % of this index was an independent significant factor for worse survival in a multivariate analyses together with age, medullary dissemination, chemotherapy and MGMT promoter methylation status (for summary see Figure 6). The prediction for patient survival could be further increased by combining this index with the MGMT promoter methylation status, showing worst patient survival for the combination of a low index together with an unmethylated MGMT promoter. As only 6 out of 227 displayed an epithelioid phenotype, the results certainly have to be considered with caution, nevertheless, the prognostic impact of such a differentiation seemed to be strongly associated with negative patient survival even in a multivariate analysis. Although a detailed definition of cell morphology is provided by the authors, the reproducibility of such an analysis with still suffer from the subjective interpretation of individual neuropathologist. If this approach should enter the diagnostic routine, future automated digital image analysis would be preferable to undoubtfully recognize and grade the morphological parameters. Figure 6: Prognostic prediction of histological features in glioblastoma
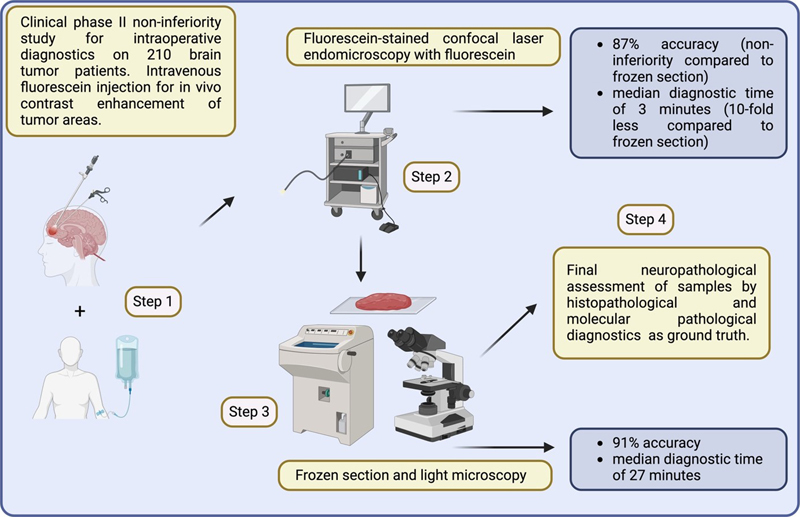
7. Confocal laser microscopy for intraoperative histopathological diagnostics of intracranial tumors [Wagner et al., 2024] Intraoperative diagnostics performed on frozen sections is time-consuming, often lasting around 20 minutes from tissue sampling out of the surgical cavity to the final transmission of the diagnosis [Novis and Zarbo, 1997]. In addition, only single, mostly very small tissue fragments can be assessed at a time. Even in highly specialized tertiary medical centers, a diagnostic shift of 18 % between intraoperative and post-operative diagnoses was reported, actually leading to a second subsequent neurosurgical intervention in 3 % of all brain tumor patients [Harms et al., 2023]. Therefore, there is an urgent need for faster methods that can also repeatedly analyze larger tissue areas, ideally in real-time and/or directly in situ. To address this issue, Wagner et al. conducted a phase II clinical study to test the noninferiority of fluorescein-stained intraoperative confocal laser endomicroscopy (CLE) compared to the classic assessment of frozen sections by neuropathologists in 210 adult brain tumor patients. CLE (using the ZEISS CONVIVO system) is a non-invasive/non-traumatic technique that enables histopathological assessment in vivo almost in real time. In addition, fluorescein sodium acts as a contrast-enhancing intraoperative dye for an easier identification of the tumor-suspicious areas. Of note, no serious adverse events were reported, neither in relation to CLE nor to fluorescein. Compared to the final neuropathological diagnoses, a correct result was obtained in 87 % of CLE-assessed samples, while classic frozen sections achieved 91 %, demonstrating the noninferiority of the CLE method (Figure 7). The concordance rate between CLE and classic frozen sections was 76 %. Most importantly, the median time until CLE diagnosis was communicated was 3 min compared to 27 min in classic frozen sections, resulting in a nearly 10-fold reduction of time required for intraoperative neuropathological assessment. In summary, in vivo CLE assessment for intraoperative neuropathological diagnostics is a highly reliable and significantly faster approach that could at least partially replace frozen section diagnostics in the future. In addition, a considerably higher amount of tissue images could be processed thereby further increasing its diagnostic validity. Figure 7
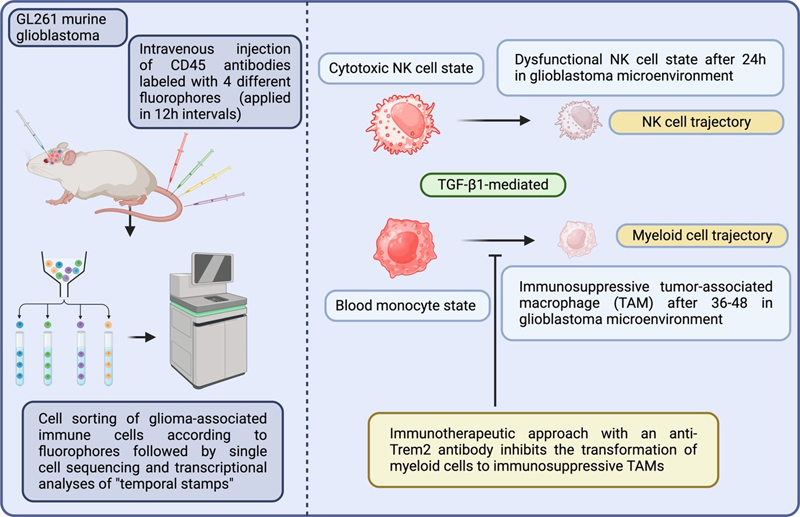
Diagnostic set-up and major results for clinical phase II non-inferiority study for intraoperative neuropathological assessment using fluorescein-stained confocal laser endomicroscopy. 8. Brain tumor diagnostics from cell-free DNA from cerebrospinal fluid [Afflerbach et al., 2024 and Hickman et al., 2024] Precise brain tumor diagnostics still relies on highly invasive procedures to obtain tissue samples for microscopic or molecular diagnostics. As high rates of intraoperative adverse events have been reported for neurosurgical interventions reaching up to 40 %, there is a strong need for non- or less invasive diagnostic procedures in neurooncology [Drexler et al., 2023a]. Ideally, a non-operative tumor classification could even prevent patients from invasive follow-up procedures as in the case of CNS lymphoma. A second important reason for why non-invasive diagnostics would considerably improve patient care would be related to the detection of early recurrences or minimal residual tumor load. Some studies have shown the suitability of sequencing techniques to detect tumor-specific mutations from cell-free DNA of the CSF in some tumor entities such as gliomas [Miller et al., 2019]. For other brain tumor entities, such as medulloblastoma, non-invasive molecular diagnostics from cell-free DNA from cerebrospinal fluid (CSF) has already been proven to be superior to cytological diagnostics with regard to both the detection of residual tumor and the prediction of patient prognosis [Liu et al., 2021]. To evaluate the suitability of molecular diagnostics on CSF-derived cell-free DNA across broader brain tumor cohorts, different research teams employed various approaches. Consequently, two exceptional papers were selected under a single topic. Afflerbach et al. analyzed a larger cohort of 110 samples from 99 patients with suspicion of primary brain tumor using Nanopore sequencing (at least 5ng DNA per sample was needed), a technique which, in addition, also considerably reduces the time needed for sample preparation and sequencing [Afflerbach et al., 2024]. In 45 % of the samples, circulating tumor DNA (ctDNA) could be detected in the CSF. Among the samples in which ctDNA was successfully detected, only the copy number variation (CNV) profile could be defined in 56 % (n = 28), only DNA methylation profiling in 12 % (n = 6), and both types of information in 32 % (n = 16). The CNV profile revealed several diagnostically relevant amplifications as well as larger chromosomal gains and losses. Of note, corresponding cytological analyses detected tumor cells in only 9 cases. With their groundbreaking study, Afflerbach et al. provided evidence that Nanopore sequencing is a fast and reliable diagnostic technique allowing for determining both CNV and DNA methylation profiles from ctDNA from CSF in brain tumor patients. In another approach, Hickman et al. performed mutational analyses of CSF circulating ctDNA from 711 brain tumor patients using an FDA-authorized targeting next-generation sequencing platform [Hickman et al., 2024]. Similarly to the findings of Afflerbach et al., also Hickman and colleagues detected tumor-specific mutations in 53 % of all patient samples with clinically documented CNS tumors, whereas none of the control samples showed a false positive result, therefore constituting a highly specific diagnostic approach. Considering the technical limitations of various approaches, nanopore-based sequencing is particularly constrained by low genomic coverage, making it unsuitable for the reliable detection of point mutations [Emiliani et al., 2025]. Moreover, since short-read next-generation sequencing techniques have successfully identified tumor-specific mutations with as little as 0.1 ng of cell-free DNA from CSF, a methodological comparison of different sequencing techniques is essential to determine the most suitable approach [Miller et al., 2022]. These approaches will considerably change our initial diagnostic approach and treatment survey in neurooncology in the future. 9. Time-dependent single-cell phenotyping of immune cells in glioblastoma [Kirschenbaum et al., 2024] Single cell RNA sequencing techniques revolutionized the understanding of individual cell states about which one could only speculate from data derived from bulk sequencing [Ramsköld et al., 2012; Tang et al., 2009]. However, it is still challenging to decipher how cell states change over time under distinct conditions, such as for example the effect of the tumor microenvironment on infiltrating immune cells. To address this question, Kirschenbaum et al. developed a new method called Zman sequencing (“Zman” is the phonetic spelling of the Hebrew word for “time”) which combines the use of fluorophore pulse labels in the blood as temporal stamps with single cell RNA sequencing [Kirschenbaum et al., 2024]. The authors intravenously applied four times an identical antibody directed against CD45 that, however, was labeled each time with a different fluorophore (n = 4 in total) in 12h intervals (between 24–60h or 12–48h before mice were sacrificed). After having confirmed that the fluorophore-coupled antibodies (a) almost exclusively stain immune cells in the blood stream, (b) can be reliably detected on immune cells over 96h, (c) do not penetrate the brain and (d) are virtually completely degraded in the blood within 60–90 min, transcriptional molecular trajectories of natural killer (NK) and myeloid cells in the syngeneic GL261 murine glioblastoma model were assessed. One can assume that CD45-positive immune cells labeled with one of the four distinct fluorophores encountering in the glioma tumor microenvironment mostly infiltrated the brain via the blood stream within a time frame of +/- 12h before the application of the next, subsequent fluorophore-labeled antibody. With this approach, a temporal transcriptional kinetic profile can be calculated for each immune cell type within the glioma microenvironment. Of note, primary microglia are mostly not stained by this approach as the intravenously injected fluorophore-coupled antibodies did not penetrate the brain. With this approach, the authors showed that NK cells changed from a cytotoxic to a dysfunctional, and myeloid cells from classic monocytes to immunosuppressive tumor-associated macrophages (TAM) via activated TGF-β1 signaling within 24h and 36–48h, respectively. As TGF-β1 signaling was associated with Trem2 activation in immune cells of the myeloid lineage, an immunotherapeutic approach with an anti-Trem2 antibody was performed in the GL261 glioma model. This treatment prevented the differentiation to immunosuppressive TAMs leading to a pro-inflammatory cell state that is supposed to possess a much stronger anti-tumoral properties by recruiting T and NK cells [Allen et al., 2017]. With their study, Kirschenbaum et al. provide a revolutionary technique allowing for deciphering the transcriptional trajectories of immune cells from the blood stream. They nicely apply this method to assess the impact of the glioma microenvironment on infiltrating immune cells showing that the tumor mostly escapes from an immune attack by inhibiting NK and myeloid cells via TGF-β1-activated pathways. Finally, they provide a smart initial therapeutic approach by preventing myeloid cells to acquire a pro-tumorigenic cell state applying an anti-Trem2 antibody (for summary see Figure 8). Figure 8: Time-dependent immune cells transcriptomics in glioblastoma.
Left side: methodological set-up. Right side: major findings of NK and myeloid cell/TAM transcriptional trajectories. 10. Histone serotonylation regulates ependymoma tumorigenesis [Chen et al., 2024] Ependymomas constitute a heterogeneous group of CNS tumors that are currently classified into at least nine distinct molecular subtypes and are partly considered an epigenetic disorder [Stuckert et al., 2020]. As recent studies have revealed a direct epigenetic modification of histone H3 by serotonin, a process termed 'serotonylation,' a potential link between serotonin-induced histone alterations and the development and progression of ependymoma has been hypothesized [Farrelly et al., 2019]. To address this hypothesis, Chen et al. generated ependymomas by performing in utero electroporation to insert the ZFTA-RELA fusion gene and knock out Trp53, a tumor suppressor gene. Additionally, a designer receptor exclusively activated by designer drugs (DREADD) approach was employed to modulate neuronal activity in cortical neurons and dorsal raphe nucleus neurons. This was achieved by injecting non-naturally occurring receptors into distinct brain areas via viral vectors, which were subsequently activated by a synthetic ligand. The authors showed that the activation of excitatory cortical neurons promoted the development of ZFTA-RELA fusion-driven ependymomas and identified serotonergic activity in the dorsal raphe nucleus – an area remote from the ependymoma – as a suppressive factor for ependymoma progression. However, established, both murine and human ependymoma cells also displayed a considerable higher amount of serotonylated H3 compared to normal CNS tissue and histone serotonylation was associated with tumor progression, providing evidence that serotonin signaling may have a rather disparate role in ependymoma tumor biology. In the experimental setting, ETS transcription variant factor 5 (ETV5), a transcription factor with binding sites for both serotonylated H3 and the ZFTA-RELA fusion, was identified as a tumor-promoting factor. The authors further demonstrated that ETV5 was associated with a repressive H3K27 trimethylation signature and decreased neuropeptide Y (NPY) expression in ependymoma. Moreover, ETV5 overexpression abrogated NPY-mediated synaptic inhibition in the tumor microenvironment, which was linked to reduced tumor growth (Figure 9). Figure 9: Disparate effects of serotonin in ependymoma tumorigenesis.
On the one hand, serotonin signaling from the dorsal raphe nucleus inhibits remote ependymoma growth, most likely by reducing neuronal activity in the tumor microenvironment. On the other hand, tumor cell-intrinsic serotonylation promotes ependymoma growth through epigenetic modification and subsequent ETV5 overexpression, ultimately leading to neuropeptide Y (NPY) inhibition. As a result, the inhibitory effect of NPY on brain activity and its tumor-suppressive function are abolished. Discussion The body of research published in 2024 reveals significant advancements in the understanding of glioblastoma and brain metastasis, with a particular emphasis on tumor heterogeneity, diagnostic advancements, and therapeutic implications. The studies covered in this overview contribute to refining our approaches to both the molecular and clinical management of brain tumors, highlighting critical challenges and innovative solutions. A major theme emerging from this year's literature is the growing recognition of the microenvironment's role in tumor progression. Roesler et al. demonstrate the pivotal impact of altered cerebral microcirculation and a hypoxic-ischemic microenvironment in the development of brain metastases [Roesler et al., 2024]. Their findings underscore the importance of understanding how changes in the vascular network and oxygen availability influence tumor spread, highlighting potential targets for therapeutic intervention, especially using prevention strategies inhibiting brain metastasis seeding by combined inhibition of VEGF and Ang-2. This approach will change our therapeutic view as oncological patients are usually treated when symptoms or lesion occur. On the primary malignant brain tumor side, Mathur et al. explored glioblastoma's evolution and heterogeneity from a whole tumor perspective [Mathur et al., 2024]. The dynamic nature of glioblastoma, with its diverse cellular populations and the continuous evolution of its genetic and epigenetic landscape, presents a substantial challenge for both diagnosis and treatment, however there is still a considerable debate about how hierarchical or rather reversible such an evolution is, the latter more speaking in favor of highly dynamic, tumor-intrinsic plasticity [Dirske et al., 2019]. DNA methylation continues to emerge as a crucial mechanism in brain tumor biology. Drexler et al. and Eckhardt et al. both highlight the significance of DNA methylation profiles in glioblastoma [Drexler et al., 2024; Eckhardt et al., 2024]. Drexler et al. demonstrate the alterations in DNA methylation in recurrent glioblastoma, providing valuable insights into the epigenetic shifts that occur during disease progression, especially that methylation classifier subclasses have to be considered with caution as they may considerably change over time. Meanwhile, Eckhardt et al. present global DNA methylation as an independent diagnostic marker for IDH-wildtype glioblastoma, offering a potential non-invasive tool for early diagnosis and prognosis. Of note, they provide an easily applicable risk score that can be integrated into routine diagnostic procedures, offering significant prognostic value by distinguishing between a high-risk group with a median survival of only 8.3 months and a low-risk group with a median survival of 39 months. These findings underscore the growing interest in epigenetic biomarkers for glioblastoma, which may ultimately improve diagnostic accuracy and allow for more personalized therapeutic strategies. In addition to DNA methylation, histopathological and molecular features are increasingly used to predict prognosis. Kirishima et al. demonstrate how histomorphological features can provide valuable prognostic information in glioblastoma, supporting the role of tissue-based diagnostics in clinical settings [Kirishima et al., 2024]. A considerable limitation of this study is that morphological criteria – despite being carefully and precisely defined – are still subject to interpretation bias. This will need to be considered in the future when using artificial intelligence algorithms applied to digital images, which are often annotated by human (neuro)pathologists during the training phase. The utilization of cutting-edge technologies such as confocal laser microscopy in intraoperative diagnostics, as outlined by Wagner et al., further enhances the speed and hopefully also the precision in the future of tumor identification and delineation, offering real-time guidance during surgery and improving patient outcomes [Wagner et al., 2024]. This technological advancement, alongside the development of non-invasive diagnostic techniques like those reported by Afflerbach et al. and Hickman et al., who used sequencing techniques of cell-free DNA from cerebrospinal fluid, marks a significant step forward in the non-invasive diagnosis and monitoring of brain tumors [Afflerbach et al., 2024; Hickman et al., 2024]. Their work presents exciting prospects for liquid biopsy as a means to detect and track tumor progression in real-time. Immune cell dynamics are also a focal point of recent studies. Kirschenbaum et al. explore the time-dependent phenotyping of immune cells in glioblastoma, providing valuable insights into the temporal changes in immune cell populations within the tumor microenvironment. These findings could have significant implications for immunotherapy, as the ability to track immune cell profiles over time may inform the development of more targeted immune-based therapies [Kirschenbaum et al., 2024]. However, at least as important as the scientific findings of this study is the technical development of tracking immune cells through time-dependent transcriptomics using the novel Zman sequencing technique. At present, this approach is primarily suited for cells infiltrating other tissue areas, previously labeled via the bloodstream. An important next step in the development of time-dependent transcriptomics would be expanding its applicability to cells that remain within a distinct cellular collective, such as brain tumor cells. This ties in with the work of Dobersalske et al., who investigated the role of cranioencephalic functional lymphoid units in glioblastoma, expanding our understanding of how immune surveillance and local immune responses may influence tumor behavior and response to treatment [Dobersalske et al., 2024]. To further decipher the temporal dynamics of 'glymphatic' drainage, Zman sequencing could also be of interest in expanding upon the findings of the study by Dobersalske et al. Finally, the role of post-translational modifications in tumorigenesis is underscored by the study of Chen et al., which examines histone serotonylation in ependymoma tumorigenesis [Chen et al., 2024]. This work highlights how serotonin-mediated alterations in histone modifications can regulate tumor growth and suggests that targeting epigenetic regulators may offer a novel therapeutic avenue for ependymomas and other brain tumors. It remains to be determined if serotonylation will be a reproducible, important factor in brain tumor progression in the future, however there is an increasing body of evidence that a crosstalk between neurons and brain tumor might be implicated [Venkataramani et al., 2025]. Together, these studies reflect a shift toward more comprehensive, multifactorial approaches to understanding and treating brain tumors. In general, there currently seems to be a disproportion between scientific studies focusing on the 'bad guys' – the brain tumor cells that proliferate, migrate, and infiltrate – and the large number of studies examining the tumor microenvironment. While the microenvironment may contribute to tumor progression, it lacks the malignant oncogenic driver mutations. It may be easier to study tumor microenvironmental factors, possibly due to superior methodological tools and simpler tracking methods, but it is crucial not to lose sight of tumor cells as the main players in future research. The integration of molecular and immune profiling, advanced imaging technologies, and epigenetic markers has the potential to revolutionize both the diagnosis and treatment of primary and secondary brain tumors. As our understanding of the complex interplay between tumor biology, the microenvironment, and the immune system deepens, we can anticipate more targeted, individualized therapies that may significantly improve patient outcomes in the future. Acknowledgements The figures were prepared using https://biorender.com figure creation tool. Single images using for the figures were freely available tagged with creative common license. Funding Statement MM would like to thank the Luxembourg National Research Fund (FNR) for the support (FNR PEARL P16/BM/11192868 grant). Conflicts of Interest The author does not have any conflict of interest to declare. Declaration of Interests The author declares no competing interests. References Afflerbach AK, Rohrandt C, Brändl B, Sönksen M, Hench J, Frank S, Börnigen D, Alawi M, Mynarek M, Winkler B, Ricklefs F, Synowitz M, Dührsen L, Rutkowski S, Wefers AK, Müller FJ, Schoof M, Schüller U. Classification of Brain Tumors by Nanopore Sequencing of Cell-Free DNA from Cerebrospinal Fluid. Clin Chem. 2024 Jan 4;70(1):250-260. https://doi.org/10.1093/clinchem/hvad115 Albuck AL, Becnel CM, Sirna DJ, Turner J. J Surg Res. 2024 Oct;302:324-328. https://doi.org/10.1016/j.jss.2024.07.021 Allen F, Bobanga ID, Rauhe P, Barkauskas D, Teich N, Tong C, Myers J, Huang AY. CCL3 augments tumor rejection and enhances CD8++ T cell infiltration through NK and CD103+ dendritic cell recruitment via IFNγ. Oncoimmunology. 2017 Nov 20;7(3):e1393598. https://doi.org/10.1080/2162402X.2017.1393598 Avraham HK, Jiang S, Fu Y, Nakshatri H, Ovadia H, Avraham S. Angiopoietin-2 mediates blood-brain barrier impairment and colonization of triple-negative breast cancer cells in brain. J Pathol. 2014 Feb;232(3):369-81. https://doi.org/10.1002/path.4304 Bohn KA, Adkins CE, Nounou MI, Lockman PR. Inhibition of VEGF and Angiopoietin-2 to Reduce Brain Metastases of Breast Cancer Burden. Front Pharmacol. 2017 Apr 11;8:193. https://doi.org/10.3389/fphar.2017.00193 Brodbelt A, Greenberg D, Winters T, Williams M, Vernon S, Collins VP; (UK) National Cancer Information Network Brain Tumour Group. Eur J Cancer. 2015 Mar;51(4):533-542. https://doi.org/10.1016/j.ejca.2014.12.014 Capper D, Jones DTW, Sill M, Hovestadt V, Schrimpf D, Sturm D, Koelsche C, Sahm F, Chavez L, Reuss DE, Kratz A, Wefers AK, Huang K, Pajtler KW, Schweizer L, Stichel D, Olar A, Engel NW, Lindenberg K, Harter PN, Braczynski AK, Plate KH, Dohmen H, Garvalov BK, Coras R, Hölsken A, Hewer E, Bewerunge-Hudler M, Schick M, Fischer R, Beschorner R, Schittenhelm J, Staszewski O, Wani K, Varlet P, Pages M, Temming P, Lohmann D, Selt F, Witt H, Milde T, Witt O, Aronica E, Giangaspero F, Rushing E, Scheurlen W, Geisenberger C, Rodriguez FJ, Becker A, Preusser M, Haberler C, Bjerkvig R, Cryan J, Farrell M, Deckert M, Hench J, Frank S, Serrano J, Kannan K, Tsirigos A, Brück W, Hofer S, Brehmer S, Seiz-Rosenhagen M, Hänggi D, Hans V, Rozsnoki S, Hansford JR, Kohlhof P, Kristensen BW, Lechner M, Lopes B, Mawrin C, Ketter R, Kulozik A, Khatib Z, Heppner F, Koch A, Jouvet A, Keohane C, Mühleisen H, Mueller W, Pohl U, Prinz M, Benner A, Zapatka M, Gottardo NG, Driever PH, Kramm CM, Müller HL, Rutkowski S, von Hoff K, Frühwald MC, Gnekow A, Fleischhack G, Tippelt S, Calaminus G, Monoranu CM, Perry A, Jones C, Jacques TS, Radlwimmer B, Gessi M, Pietsch T, Schramm J, Schackert G, Westphal M, Reifenberger G, Wesseling P, Weller M, Collins VP, Blümcke I, Bendszus M, Debus J, Huang A, Jabado N, Northcott PA, Paulus W, Gajjar A, Robinson GW, Taylor MD, Jaunmuktane Z, Ryzhova M, Platten M, Unterberg A, Wick W, Karajannis MA, Mittelbronn M, Acker T, Hartmann C, Aldape K, Schüller U, Buslei R, Lichter P, Kool M, Herold-Mende C, Ellison DW, Hasselblatt M, Snuderl M, Brandner S, Korshunov A, von Deimling A, Pfister SM. DNA methylation-based classification of central nervous system tumours. Nature. 2018 Mar 22;555(7697):469-474. https://doi.org/10.1038/nature26000 Chen HC, He P, McDonald M, Williamson MR, Varadharajan S, Lozzi B, Woo J, Choi DJ, Sardar D, Huang-Hobbs E, Sun H, Ippagunta SM, Jain A, Rao G, Merchant TE, Ellison DW, Noebels JL, Bertrand KC, Mack SC, Deneen B. Histone serotonylation regulates ependymoma tumorigenesis. Nature. 2024 Aug;632(8026):903-910. https://doi.org/10.1038/s41586-024-07751-z Choi HJ, Choi SH, You SH, Yoo RE, Kang KM, Yun TJ, Kim JH, Sohn CH, Park CK, Park SH. MGMT Promoter Methylation Status in Initial and Recurrent Glioblastoma: Correlation Study with DWI and DSC PWI Features. AJNR Am J Neuroradiol. 2021 May;42(5):853-860. https://doi.org/10.3174/ajnr.A7004 Dejaegher J, Solie L, Hunin Z, Sciot R, Capper D, Siewert C, Van Cauter S, Wilms G, van Loon J, Ectors N, Fieuws S, Pfister SM, Van Gool SW, De Vleeschouwer S. Neuro Oncol. 2021 Feb 25;23(2):240-250. https://doi.org/10.1093/neuonc/noaa247 Dirkse A, Golebiewska A, Buder T, Nazarov PV, Muller A, Poovathingal S, Brons NHC, Leite S, Sauvageot N, Sarkisjan D, Seyfrid M, Fritah S, Stieber D, Michelucci A, Hertel F, Herold-Mende C, Azuaje F, Skupin A, Bjerkvig R, Deutsch A, Voss-Böhme A, Niclou SP. Stem cell-associated heterogeneity in Glioblastoma results from intrinsic tumor plasticity shaped by the microenvironment. Nat Commun. 2019 Apr 16;10(1):1787. https://doi.org/10.1038/s41467-019-09853-z Dobersalske C, Rauschenbach L, Hua Y, Berliner C, Steinbach A, Grüneboom A, Kokkaliaris KD, Heiland DH, Berger P, Langer S, Tan CL, Stenzel M, Landolsi S, Weber F, Darkwah Oppong M, Werner RA, Gull H, Schröder T, Linsenmann T, Buck AK, Gunzer M, Stuschke M, Keyvani K, Forsting M, Glas M, Kipnis J, Steindler DA, Reinhardt HC, Green EW, Platten M, Tasdogan A, Herrmann K, Rambow F, Cima I, Sure U, Scheffler B. Cranioencephalic functional lymphoid units in glioblastoma. Nat Med. 2024 Oct;30(10):2947-2956. https://doi.org/10.1038/s41591-024-03152-x Drexler R, Khatri R, Schüller U, Eckhardt A, Ryba A, Sauvigny T, Dührsen L, Mohme M, Ricklefs T, Bode H, Hausmann F, Huber TB, Bonn S, Voß H, Neumann JE, Silverbush D, Hovestadt V, Suvà ML, Lamszus K, Gempt J, Westphal M, Heiland DH, Hänzelmann S, Ricklefs FL. Temporal change of DNA methylation subclasses between matched newly diagnosed and recurrent glioblastoma. Acta Neuropathol. 2024 Jan 20;147(1):21. https://doi.org/10.1007/s00401-023-02677-8 Drexler R, Ricklefs FL, Pantel T, Göttsche J, Nitzschke R, Zöllner C, Westphal M, Dührsen L. Acta Neurochir (Wien). 2023a Aug;165(8):2015-2027. https://doi.org/10.1007/s00701-023-05672-w Drexler R, Schüller U, Eckhardt A, Filipski K, Hartung TI, Harter PN, Divé I, Forster MT, Czabanka M, Jelgersma C, Onken J, Vajkoczy P, Capper D, Siewert C, Sauvigny T, Lamszus K, Westphal M, Dührsen L, Ricklefs FL. Neuro Oncol. 2023b Feb 14;25(2):315-325. https://doi.org/10.1093/neuonc/noac177. Eckhardt A, Drexler R, Schoof M, Struve N, Capper D, Jelgersma C, Onken J, Harter PN, Weber KJ, Divé I, Rothkamm K, Hoffer K, Klumpp L, Ganser K, Petersen C, Ricklefs F, Kriegs M, Schüller U. Mean global DNA methylation serves as independent prognostic marker in IDH-wildtype glioblastoma. Neuro Oncol. 2024 Mar 4;26(3):503-513. https://doi.org/10.1093/neuonc/noad197 Emiliani FE, Ismail AAO, Hughes EG, Tsongalis GJ, Zanazzi GJ, Lin CC. Nanopore-based random genomic sampling for intraoperative molecular diagnosis. Genome Med. 2025 Jan 20;17(1):6. https://doi.org/10.1186/s13073-025-01427-7 Farrelly LA, Thompson RE, Zhao S, Lepack AE, Lyu Y, Bhanu NV, Zhang B, Loh YE, Ramakrishnan A, Vadodaria KC, Heard KJ, Erikson G, Nakadai T, Bastle RM, Lukasak BJ, Zebroski H 3rd, Alenina N, Bader M, Berton O, Roeder RG, Molina H, Gage FH, Shen L, Garcia BA, Li H, Muir TW, Maze I. Nature. 2019 Mar;567(7749):535-539. https://doi.org/10.1038/s41586-019-1024-7 Harms JWA, Streckert EMS, Kiolbassa NM, Thomas C, Grauer O, Oertel M, Eich HT, Stummer W, Paulus W, Brokinkel B. Confounders of intraoperative frozen section pathology during glioma surgery. Neurosurg Rev. 2023 Oct 28;46(1):286. https://doi.org/10.1007/s10143-023-02169-z Hickman RA, Miller AM, Holle BM, Jee J, Liu SY, Ross D, Yu H, Riely GJ, Ombres C, Gewirtz AN, Reiner AS, Nandakumar S, Price A, Kaley TJ, Graham MS, Vanderbilt C, Rana S, Hill K, Chabot K, Campos C, Nafa K, Shukla N, Karajannis M, Li B, Berger M, Ladanyi M, Pentsova E, Boire A, Brannon AR, Bale T, Mellinghoff IK, Arcila ME. Real-world experience with circulating tumor DNA in cerebrospinal fluid from patients with central nervous system tumors. Acta Neuropathol Commun. 2024 Sep 17;12(1):151. https://doi.org/10.1186/s40478-024-01846-4 Kienast Y, von Baumgarten L, Fuhrmann M, Klinkert WE, Goldbrunner R, Herms J, Winkler F. Real-time imaging reveals the single steps of brain metastasis formation. Nat Med. 2010 Jan;16(1):116-22. https://doi.org/10.1038/nm.2072 Kirishima M, Yokoyama S, Akahane T, Higa N, Uchida H, Yonezawa H, Matsuo K, Yamamoto J, Yoshimoto K, Hanaya R, Tanimoto A. Prognosis prediction via histological evaluation of cellular heterogeneity in glioblastoma. Sci Rep. 2024 Oct 23;14(1):24955. https://doi.org/10.1038/s41598-024-76826-8 Kirschenbaum D, Xie K, Ingelfinger F, Katzenelenbogen Y, Abadie K, Look T, Sheban F, Phan TS, Li B, Zwicky P, Yofe I, David E, Mazuz K, Hou J, Chen Y, Shaim H, Shanley M, Becker S, Qian J, Colonna M, Ginhoux F, Rezvani K, Theis FJ, Yosef N, Weiss T, Weiner A, Amit I. Time-resolved single-cell transcriptomics defines immune trajectories in glioblastoma. Cell. 2024 Jan 4;187(1):149-165.e23. https://doi.org/10.1016/j.cell.2023.11.032 Kovalchuk B, Berghoff AS, Karreman MA, Frey K, Piechutta M, Fischer M, Grosch J, Heiland S, Breckwoldt MO, Hilberg F, Wick W, Winkler F. Nintedanib and a bi-specific anti-VEGF/Ang2 nanobody selectively prevent brain metastases of lung adenocarcinoma cells. Clin Exp Metastasis. 2020 Dec;37(6):637-648. https://doi.org/10.1007/s10585-020-10055-x Liu APY, Smith KS, Kumar R, Paul L, Bihannic L, Lin T, Maass KK, Pajtler KW, Chintagumpala M, Su JM, Bouffet E, Fisher MJ, Gururangan S, Cohn R, Hassall T, Hansford JR, Klimo P Jr, Boop FA, Stewart CF, Harreld JH, Merchant TE, Tatevossian RG, Neale G, Lear M, Klco JM, Orr BA, Ellison DW, Gilbertson RJ, Onar-Thomas A, Gajjar A, Robinson GW, Northcott PA. Serial assessment of measurable residual disease in medulloblastoma liquid biopsies. Cancer Cell. 2021 Nov 8;39(11):1519-1530.e4. https://doi.org/10.1016/j.ccell.2021.09.012 Mallick S, Benson R, Venkatesulu B, Melgandi W, Rath GK. Systematic Review and Individual Patient Data Analysis of Uncommon Variants of Glioblastoma: An Analysis of 196 Cases. Neurol India. 2022 Sep-Oct;70(5):2086-2092. https://doi.org/10.4103/0028-3886.359222 Mathur R, Wang Q, Schupp PG, Nikolic A, Hilz S, Hong C, Grishanina NR, Kwok D, Stevers NO, Jin Q, Youngblood MW, Stasiak LA, Hou Y, Wang J, Yamaguchi TN, Lafontaine M, Shai A, Smirnov IV, Solomon DA, Chang SM, Hervey-Jumper SL, Berger MS, Lupo JM, Okada H, Phillips JJ, Boutros PC, Gallo M, Oldham MC, Yue F, Costello JF. Glioblastoma evolution and heterogeneity from a 3D whole-tumor perspective. Cell. 2024 Jan 18;187(2):446-463.e16. https://doi.org/10.1016/j.cell.2023.12.013 Mikkelsen VE, Solheim O, Salvesen Ø, Torp SH. The histological representativeness of glioblastoma tissue samples. Acta Neurochir (Wien). 2021 Jul;163(7):1911-1920. https://doi.org/10.1007/s00701-020-04608-y Miller AM, Shah RH, Pentsova EI, Pourmaleki M, Briggs S, Distefano N, Zheng Y, Skakodub A, Mehta SA, Campos C, Hsieh WY, Selcuklu SD, Ling L, Meng F, Jing X, Samoila A, Bale TA, Tsui DWY, Grommes C, Viale A, Souweidane MM, Tabar V, Brennan CW, Reiner AS, Rosenblum M, Panageas KS, DeAngelis LM, Young RJ, Berger MF, Mellinghoff IK. Tracking tumour evolution in glioma through liquid biopsies of cerebrospinal fluid. Nature. 2019 Jan;565(7741):654-658. https://doi.org/10.1038/s41586-019-0882-3 Miller AM, Szalontay L, Bouvier N, Hill K, Ahmad H, Rafailov J, Lee AJ, Rodriguez-Sanchez MI, Yildirim O, Patel A, Bale TA, Benhamida JK, Benayed R, Arcila ME, Donzelli M, Dunkel IJ, Gilheeney SW, Khakoo Y, Kramer K, Sait SF, Greenfield JP, Souweidane MM, Haque S, Mauguen A, Berger MF, Mellinghoff IK, Karajannis MA. Next-generation sequencing of cerebrospinal fluid for clinical molecular diagnostics in pediatric, adolescent and young adult brain tumor patients. Neuro Oncol. 2022 Oct 3;24(10):1763-1772. https://doi.org/10.1093/neuonc/noac035 Mittelbronn M. Neurooncology: 2023 update. Free Neuropathol. 2023 Mar 20;4:4-4. https://doi.org/10.17879/freeneuropathology-2023-4692. Mittelbronn M. Neurooncology: 2024 update. Free Neuropathol. 2024 Sep 27;5:21. https://doi.org/10.17879/freeneuropathology-2024-5809. Novis DA, Zarbo RJ. Interinstitutional comparison of frozen section turnaround time. A College of American Pathologists Q-Probes study of 32868 frozen sections in 700 hospitals. Arch Pathol Lab Med. 1997 Jun;121(6):559-67. PMID: 9199619 Puchalski RB, Shah N, Miller J, Dalley R, Nomura SR, Yoon JG, Smith KA, Lankerovich M, Bertagnolli D, Bickley K, Boe AF, Brouner K, Butler S, Caldejon S, Chapin M, Datta S, Dee N, Desta T, Dolbeare T, Dotson N, Ebbert A, Feng D, Feng X, Fisher M, Gee G, Goldy J, Gourley L, Gregor BW, Gu G, Hejazinia N, Hohmann J, Hothi P, Howard R, Joines K, Kriedberg A, Kuan L, Lau C, Lee F, Lee H, Lemon T, Long F, Mastan N, Mott E, Murthy C, Ngo K, Olson E, Reding M, Riley Z, Rosen D, Sandman D, Shapovalova N, Slaughterbeck CR, Sodt A, Stockdale G, Szafer A, Wakeman W, Wohnoutka PE, White SJ, Marsh D, Rostomily RC, Ng L, Dang C, Jones A, Keogh B, Gittleman HR, Barnholtz-Sloan JS, Cimino PJ, Uppin MS, Keene CD, Farrokhi FR, Lathia JD, Berens ME, Iavarone A, Bernard A, Lein E, Phillips JW, Rostad SW, Cobbs C, Hawrylycz MJ, Foltz GD. An anatomic transcriptional atlas of human glioblastoma. Science. 2018 May 11;360(6389):660-663. https://doi.org/10.1126/science.aaf2666 Ramsköld D, Luo S, Wang YC, Li R, Deng Q, Faridani OR, Daniels GA, Khrebtukova I, Loring JF, Laurent LC, Schroth GP, Sandberg R. Full-length mRNA-Seq from single-cell levels of RNA and individual circulating tumor cells. Nat Biotechnol. 2012 Aug;30(8):777-82. https://doi.org/10.1038/nbt.2282 Roesler J, Spitzer D, Jia X, Aasen SN, Sommer K, Roller B, Olshausen N, Hebach NR, Albinger N, Ullrich E, Zhu L, Wang F, Macas J, Forster MT, Steinbach JP, Sevenich L, Devraj K, Thorsen F, Karreman MA, Plate KH, Reiss Y, Harter PN. Disturbance in cerebral blood microcirculation and hypoxic-ischemic microenvironment are associated with the development of brain metastasis. Neuro Oncol. 2024 Nov 4;26(11):2084-2099. https://doi.org/10.1093/neuonc/noae094 Smyth LCD, Xu D, Okar SV, Dykstra T, Rustenhoven J, Papadopoulos Z, Bhasiin K, Kim MW, Drieu A, Mamuladze T, Blackburn S, Gu X, Gaitán MI, Nair G, Storck SE, Du S, White MA, Bayguinov P, Smirnov I, Dikranian K, Reich DS, Kipnis J. Identification of direct connections between the dura and the brain Nature. 2024 Mar;627(8002):165-173. https://doi.org/10.1038/s41586-023-06993-7 Stuckert A, Bertrand KC, Wang P, Smith A, Mack SC. Weighing ependymoma as an epigenetic disease. J Neurooncol. 2020 Oct;150(1):57-61. https://doi.org/10.1007/s11060-020-03562-0 Tang F, Barbacioru C, Wang Y, Nordman E, Lee C, Xu N, Wang X, Bodeau J, Tuch BB, Siddiqui A, Lao K, Surani MA. mRNA-Seq whole-transcriptome analysis of a single cell. Nat Methods. 2009 May;6(5):377-82. https://doi.org/10.1038/nmeth.1315 Venkataramani V, Yang Y, Ille S, Suchorska B, Loges S, Tost H, Sahm F, Pfister SM, Trumpp A, Krieg SM, Kuner T, Wick W, Winkler F. Cancer Neuroscience of Brain Tumors: From Multicellular Networks to Neuroscience-Instructed Cancer Therapies. Cancer Discov. 2025 Jan 13;15(1):39-51. https://doi.org/10.1158/2159-8290.CD-24-0194 Verhaak RG, Hoadley KA, Purdom E, Wang V, Qi Y, Wilkerson MD, Miller CR, Ding L, Golub T, Mesirov JP, Alexe G, Lawrence M, O'Kelly M, Tamayo P, Weir BA, Gabriel S, Winckler W, Gupta S, Jakkula L, Feiler HS, Hodgson JG, James CD, Sarkaria JN, Brennan C, Kahn A, Spellman PT, Wilson RK, Speed TP, Gray JW, Meyerson M, Getz G, Perou CM, Hayes DN; Cancer Genome Atlas Research Network. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell. 2010 Jan 19;17(1):98-110. https://doi.org/10.1016/j.ccr.2009.12.020 Wagner A, Brielmaier MC, Kampf C, Baumgart L, Aftahy AK, Meyer HS, Kehl V, Höhne J, Schebesch KM, Schmidt NO, Zoubaa S, Riemenschneider MJ, Ratliff M, Enders F, von Deimling A, Liesche-Starnecker F, Delbridge C, Schlegel J, Meyer B, Gempt J. Fluorescein-stained confocal laser endomicroscopy versus conventional frozen section for intraoperative histopathological assessment of intracranial tumors. Neuro Oncol. 2024 May 3;26(5):922-932. https://doi.org/10.1093/neuonc/noae006 World Health Organization Classification of Tumours of the Central Nervous System. 5th ed. Lyon: International Agency for Research on Cancer; 2021. https://doi.org/10.1093/neuonc/noab106
Copyright: © 2025 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |