|
|
|
Free Neuropathology 5:25 (2024) |
|
Letter |
|
Infantile pilocytic astrocytoma with persisting external granular layer of the cerebellum: a potential diagnostic pitfall |
|
Arnault Tauziède-Espariat1,2, Lauren Hasty1, Alice Métais1,2, Pascale Varlet1,2 |
|
|
Corresponding author: |
|
Submitted: 15 September 2024 |
|
Keywords: Pilocytic astrocytoma, External granular layer, Dysplasia |
|
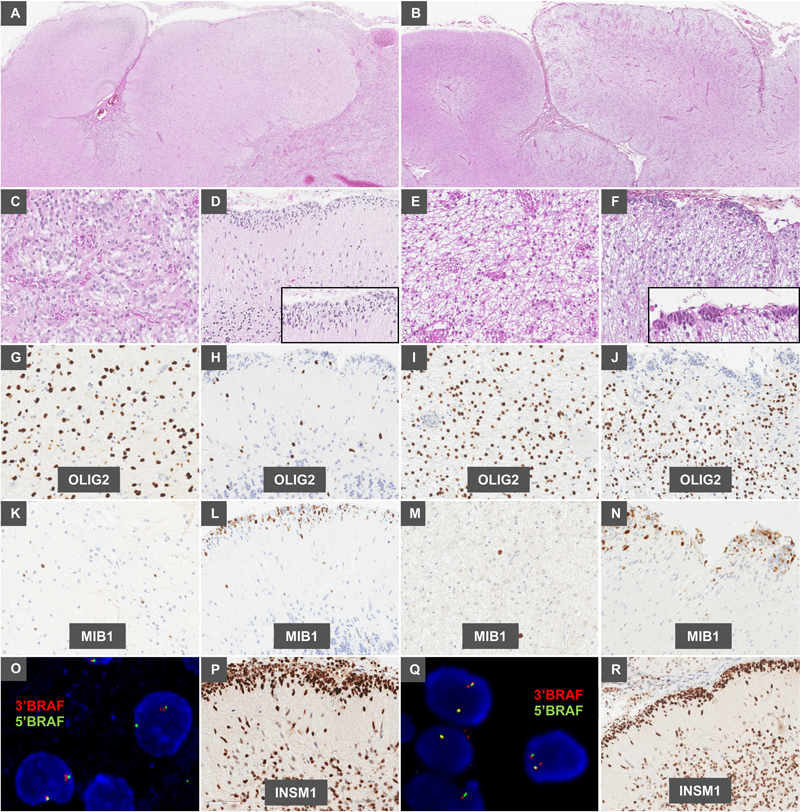
Introduction Pilocytic astrocytomas (PA) are frequent astrocytic neoplasms that generally have a circumscribed architecture. They are molecularly characterized by MAPK gene pathway alterations, mostly KIAA1549::BRAF fusions (1). PA affect children along the neuraxis, but are typically found in the posterior fossa (2). Dysplastic modifications of the brain parenchyma have been described as being associated with epileptic supratentorial tumors (3,4). In the cerebellum, the gangliocytoma (known as “Lhermitte-Duclos disease”), which is generally a symptom of Cowden syndrome, is defined by typical radiological and histopathological features (5,6). It is characterized by a distorted architecture with enlarged cerebellar folia containing dysplastic ganglion cells and a diffuse enlargement of the molecular and internal granular layers (6). Whereas it is mainly reported in adults, it can be discovered during childhood (7). Herein, we report two cases of young children presenting PA associated with major dysplastic modifications of the adjacent cerebellar parenchyma. Case presentation The two cases concerned infants (two boys, 11 and 18 months respectively) who presented a cerebellar mass which was grossly resected. Both tumors exhibited features of PA (Figure 1 A-B, C and E). Indeed, each tumor was biphasic with piloid and oligodendrocyte-like cells, had low to moderate cellularity and a significant amount of Rosenthal fibers. There were no eosinophilic granular bodies, perivascular lymphocytic infiltrates, binucleated ganglion cells or neuropil-like islands. Tumor cells did not present atypia and mitotic figures were scarce. Glomeruloid microvascular proliferation was observed. The tumors were solid and diffuse, and peripherally infiltrated the adjacent parenchyma. On the surface of the cerebellar folia, clusters of small undifferentiated blue cells with round hyperchromatic nuclei and mitoses were present, and their cytoplasm was loosely abundant. Using immunohistochemistry, the tumor cells of PA expressed OLIG2 (Figure G and I) and GFAP, and were not immunopositive for neuronal markers (such as chromogranin A, synaptophysin, NeuN, or INSM1). The expression of H3K27me3 and IN1I was retained. CD34 immunostaining highlighted the vascularization without extravascular expression. No necrosis was observed and the MIB1 labeling index was low (1–2%) (Figure 1K and M). The small cell component was only immunoreactive for INSM1 (Figure 1H, J, P and R) and the MIB1 labeling index was high in these areas (Figure 1L and N). The FISH (Fluorescent in situ Hybridization) analysis of the BRAF locus identified a rearrangement of tumor cells in both cases (Figure 1O and Q) without abnormality in the superficial undifferentiated cells. FISH did not reveal a 1p deletion for either case. A final diagnosis of PA of the posterior fossa, BRAF-rearranged associated with “dysplastic” modifications of the adjacent cerebellar parenchyma and the persistence of the external granular layer was suggested. Fourteen and four years after the initial diagnoses, both patients were alive without tumor residue or recurrence.
Figure 1. Histological and molecular features of the two cases Case #1 (A, C, D, G, H, K, L, O and P) and Case #2 (B, E, F, I, J, M, N, Q and R). (A and B) Atrophy of the folia of the cerebellum with a lowly cellular proliferation (HPS, magnification x40). (C and E) The tumor was composed of astrocytic cells with a piloid appearance (HPS, magnification x400). (D and F) At the surface, there was a subpial proliferation of small immature cells (HPS, magnification x400 and 600 for inserts). (G and I) Tumor cells diffusely expressed OLIG2 whereas superficial immature cells did not (H and J) (magnification x400). The proliferation index was low in both tumors (K and M) whereas it was high in the superficial immature component (L and N). (O and Q) A rearrangement of the BRAF gene was evidenced in tumor cells of the pilocytic astrocytomas with a duplication of the 3’BRAF signal, and was absent in the immature component (data not shown) (magnification x800). (P and R) The superficial cell component diffusely expressed INSM1, an immature neuronal marker (magnification x400). HPS: Hematoxylin Phloxin Saffron. Discussion and conclusions The mature cerebellar cortex is composed of three layers: the upper layer (stratum moleculare) containing a small amount of neurons (basket neurons and small stellate neurons), a middle layer (stratum gangliosum) where Purkinje cells are found, and the deepest layer (stratum granulosum) comprised of tiny neurons (granule cells) and Golgi cells (8,9). During the development of the cerebellum, is has been shown that granule cell precursors proliferate in the external granular layer and migrate through the molecular layer to the internal granular layer (8). Subsequently, during the late postnatal period (2–8 months), there is a slow decrease in the width of the external granular layer which disappears between the eighth and eleventh months (8). The two current cases illustrate the development of PA during the early life of two infants. The persistence of the external granular layer of the cerebellar parenchyma suggests that the formation of the tumors may have started before 2–8 months of life or before birth. These immature neurons, which normally disappear after childbirth, constitute a histopathological diagnostic pitfall, which could possibly be confused with an embryonal tumor or an undifferentiated tumor component. This is particularly confusing because these immature neurons present high mitotic and proliferative indexes. However, these cells have a peculiar position, aligned at the surface of the cerebellar parenchyma. Using immunohistochemistry, they only expressed INSM1, a marker of immature neurons (10). Moreover, the absence of the BRAF rearrangement, which was identified in the adjacent PA, argues against a poorly differentiated component. In rare cases, PA can present a rhythmic palisaded pattern, previously referred to as spongioblastoma, in reference to polar spongioblasts (neuroectodermal cells known to initiate the differentiation of radial glial cells) (11), which was not observed in the current cases. Pilocytic astrocytomas represent the most common form of pediatric glioma and may occur in rare infantile cases (12). The persistence of an external granular layer of the cerebellum differs from the features of Lhermitte-Duclos disease where the cerebellar folia are replaced by large ganglion cells and inner granule cells are absent (6). In conclusion, the persistence of an external granular layer of the cerebellum may occur in cases with antenatal/perinatal tumor development and is not to be confused with embryonal/poorly differentiated neoplastic cells. Declarations Ethics approval This study was approved by GHU Paris Psychiatry and Neuroscience, Sainte-Anne Hospital’s local ethics committee. Consent for publication The legal guardians signed informed consent forms before treatment. Conflicts of interest Statement The authors declare that they have no conflicts of interest directly related to the topic of this article. Funding Statement The authors declare that they have not received any funding. Acknowledgements We would like to thank the laboratory technicians at GHU Paris Neuro Sainte-Anne for their assistance. References 1. Jones DTW, Kocialkowski S, Liu L, Pearson DM, Bäcklund LM, Ichimura K, et al. Tandem duplication producing a novel oncogenic BRAF fusion gene defines the majority of pilocytic astrocytomas. Cancer Res. 2008;68(21):8673–7. 2. Collins VP, Jones DTW, Giannini C. Pilocytic astrocytoma: pathology, molecular mechanisms and markers. Acta Neuropathol (Berl). 2015;129(6):775–88. https://doi.org/10.1007/s00401-015-1410-7 3. Blümcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, et al. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia. 2011;52(1):158–74. https://doi.org/10.1111/j.1528-1167.2010.02777 4. Oda M, Arai N, Maehara T, Shimizu H, Kojima H, Yagishita A. Brain tumors in surgical neuropathology of intractable epilepsies, with special reference to cerebral dysplasias. Brain Tumor Pathol. 1998;15(1):41–51. https://doi.org/10.1007/BF02482100 5. Wei G, Zhang W, Li Q, Kang X, Zhao H, Liu X, et al. Magnetic resonance characteristics of adult-onset Lhermitte-Duclos disease: An indicator for active cancer surveillance? Mol Clin Oncol. 2014;2(3):415–20. https://doi.org/10.3892/mco.2014.258 6. Abel TW, Baker SJ, Fraser MM, Tihan T, Nelson JS, Yachnis AT, et al. Lhermitte-Duclos disease: a report of 31 cases with immunohistochemical analysis of the PTEN/AKT/mTOR pathway. J Neuropathol Exp Neurol. 2005;64(4):341–9. 7. Longy M, Lacombe D. Cowden disease. Report of a family and review. Ann Genet. 1996;39(1):35–42. PMID: 9297442 8. Abrahám H, Tornóczky T, Kosztolányi G, Seress L. Cell formation in the cortical layers of the developing human cerebellum. Int J Dev Neurosci. 2001;19(1):53–62. https://doi.org/10.1016/s0736-5748(00)00065-4 9. Rakic P, Sidman RL. Histogenesis of cortical layers in human cerebellum, particularly the lamina dissecans. J Comp Neurol. 1970;139(4):473–500. https://doi.org/10.1002/cne.901390407 10. Duggan A, Madathany T, de Castro SCP, Gerrelli D, Guddati K, García-Añoveros J. Transient expression of the conserved zinc finger gene INSM1 in progenitors and nascent neurons throughout embryonic and adult neurogenesis. J Comp Neurol. 2008;507(4):1497–520. https://doi.org/10.1002/cne.21629 11. Schiffer D, Cravioto H, Giordana MT, Migheli A, Pezzulo T, Vigliani MC. Is polar spongioblastoma a tumor entity? J Neurosurg. 1993;78(4):587–91. https://doi.org/10.3171/jns.1993.78.4.0587 12. Tauziède-Espariat A, Beccaria K, Dangouloff-Ros V, Sievers P, Meurgey A, Pissaloux D, et al. A comprehensive analysis of infantile central nervous system tumors to improve distinctive criteria for infant-type hemispheric glioma versus desmoplastic infantile ganglioglioma/astrocytoma. Brain Pathol. 2023;e13182. https://doi.org/10.1111/bpa.13182
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |