|
|
|
Free Neuropathology 5:28 (2024) |
|
Letter |
|
Glioneuronal heterotopia in the right middle cranial fossa |
|
Emilie Russler-Germain1, Shamaita Majumdar2, Theresa Nguyen2, Keiko Hirose3, Peter H. Yang4, Ali Mian2, Sonika Dahiya1 |
|
|
Corresponding author: |
|
Submitted: 05 September 2024 |
|
Keywords: Glioneuronal heterotopia, Intracranial extracerebral, Pigmented ocular epithelium, Choroid plexus |
|
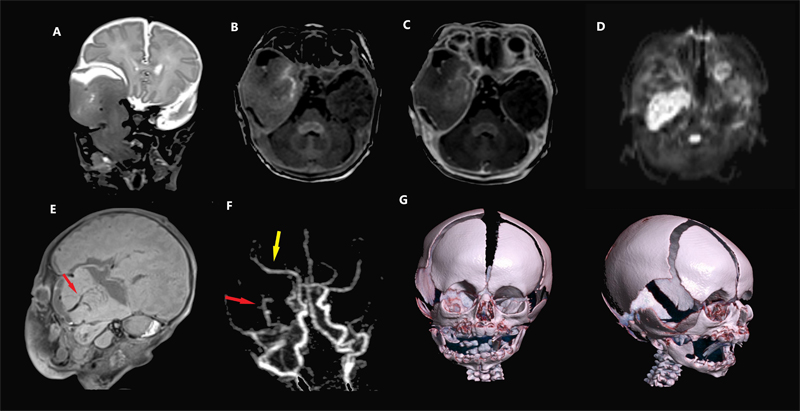
A newborn boy, delivered vaginally at 40 weeks and 2 days gestation at home under the care of a midwife to a 28-year-old gravida 2 para 2 mother, was noted to have bleeding from his oral cavity at birth. Prenatal care was adequate and the pregnancy was uncomplicated, with no concerning findings noted on 20-week ultrasound. The patient was brought to the hospital for evaluation and was admitted to the neonatal intensive care unit. The pediatric otolaryngology service was consulted, and examination revealed fullness of the right temporal fossa with absence of a portion of the squamous temporal bone. A mass of the right oropharynx was noted directly posterior to the tonsil, and the soft palate and uvula were asymmetric, resembling a shallow cleft. Despite this, the patient was breathing comfortably without evidence of respiratory distress. Magnetic resonance imaging (MRI) of the skull base revealed a large cystic and solid extra-axial mass in the right middle cranial fossa, displacing the right temporal lobe and extending into the right infratemporal fossa through a large skull base defect, as well as cleft palate. Furthermore, the mass protruded into the oropharynx (Figure 1A). The adjacent brain parenchyma appeared radiologically separate from the mass. The mass had signal intensity resembling brain parenchyma except for faint enhancement at the center and diffusion restriction in the infratemporal component (Figure 1B–D). The vascular supply of this mass appeared separate from the adjacent brain with its own feeding vessel and distal perfusion (Figure 1E–F). MRI sequences demonstrating diffusion restriction suggested this lesion could represent a malignancy. However, the lesion did not invade adjacent structures and appeared to induce bony erosion not by infiltration but by resorption and remodeling (Figure 1G). Therefore, a benign diagnosis was favored.
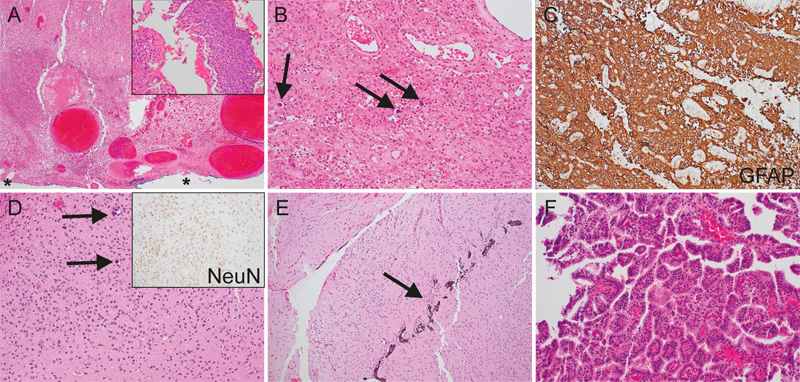
Figure 1. Head and neck imaging. Coronal T2 MRI (A) shows a mass extending from the middle cranial fossa through a skull base defect into the right infratemporal fossa. The adjacent normal brain parenchyma is displaced but not involved by the mass, with a clear cerebrospinal fluid (CSF) cleft separating the two. Axial pre-contrast (B) and post-contrast (C) T1 MPRAGE images show minimal enhancement at the center, but the majority of the mass is non-enhancing. Axial diffusion-weighted imaging (D) shows diffusion restriction in the infratemporal mass, suggestive of hypercellularity, a feature often concerning for an aggressive tumor, though this can also be seen in benign lesions. Sagittal T1 SPACE MRI (E) and post-contrast MRA (F) show a prominent vascular pedicle (red arrows) in the center of the mass and the displaced right middle cerebral artery (yellow arrow). 3D renderings of the skull (G) show budging of the squamosal temporal bone and widening of the suture rather than osseous destruction. On day 4 of life, the patient underwent transoral biopsy of the oropharyngeal portion of the mass. On days 18 and 33 of life, the patient underwent staged debulking of the intracranial and right orbital components with reservoir placement and covering of the skull base defect due to concern for progressive intracranial mass effect. Intraoperatively, the mass was noted to respond to surgical manipulation with consistency akin to normal brain parenchyma. The patient was discharged home on day 44 of life in good condition. Histopathological analysis of the mass revealed fragments of malformed, disorganized glioneuronal tissue with calcospherites and perivascular dystrophic calcifications, as well as, reactive changes including gliosis. In addition, few detached fragments of unremarkable choroid plexus and foci of pigmented ocular epithelium were notable (Figure 2). Minuscule fragments were suggestive of putative ependymal lining and meningeal tissue. The final histological diagnosis was consistent with intracranial extracerebral glioneuronal heterotopia (IEGH) with oropharyngeal extension. Developing brain tissue and robust reactive changes resulted in high proliferation indices, a potential diagnostic pitfall. The differential possibility of teratoma was ruled out due to lack of endodermal components.
Figure 2. Histopathological analysis. Oropharyngeal biopsy (A–C): Low- (A) and high- (B) power hematoxylin and eosin-stained sections demonstrate widespread ulceration (*) of the lining squamous epithelium (inset), hyalinized ectatic vessels, and reactive glioneuronal tissue (arrows indicate calcospherites). Glial fibrillary acidic protein (GFAP) confirms a dominant glial component (C). Resection of the intracranial mass (D-F) further substantiates the malformed nature of the glioneuronal tissue (D, arrows indicate calcospherites; inset highlights the disorganized arrangement of neurons by NeuN immunostaining), as well as, pigmented ocular epithelium (arrow, E) and unremarkable fragments of choroid plexus (F). Whole exome sequencing and RNA-sequencing of the oropharyngeal biopsy were performed by Caris Life Sciences. Whole exome sequencing revealed no pathogenic gene alterations or whole arm chromosomal alterations. A number of variants of uncertain significance and unclassified gene variants with variant allele frequencies approximating 50 % were detected, suggestive of germline alterations. Additionally, uncharacterized fusions of UMAD1::GLCCI1 and KANSL1::ARL17A were detected through RNA-sequencing, the significances of which are unclear but which are possibly germline1. Karyotype analysis, performed using whole exome sequencing, identified duplications of the centromeric portion of chromosome 22, as well as the distal portion of chromosome 22q. No chromosomal losses were detected. Microsatellite status was stable, genomic loss of heterozygosity was 1 %, and tumor mutational burden was 2 mutations / megabase (MB). Overall, the genetic analyses were consistent with a non-neoplastic process. The term glioneuronal heterotopia / ectopia encompasses microscopic, small nodular or large mass-like ectopic neuroectodermal tissue, both within or outside of the neuraxis2. A well-recognized example of ectopic glioneuronal tissue is the intranasal or extranasal “nasal glioma”2–5. Intraparenchymal, dural / leptomeningeal, intracranial extracerebral, and “distal” (e.g. orbit, palate, middle ear, internal auditory canal, oral cavity, oropharynx, and lung) locations are also possible2,3,6–8. Mass-like glioneuronal heterotopias are uncommon developmental malformations and can be difficult to distinguish from primary central nervous system (CNS) neoplasms on radiologic and pathologic evaluation. While microscopic glioneuronal heterotopia likely result from aberrant glial and neuronal migration9, the pathogenesis of large mass-like glioneuronal heterotopia is less well understood. Possible etiologies include aberrant sequestration of embryonic tissue during development with subsequent dysregulated growth versus encephalocele with obliteration of the connecting stalk5. IEGH most commonly occurs in the middle cranial fossa, with fewer than 20 cases reported in the literature and even fewer reports of extracranial extension2,3,6,10–23. Literature review of published IEGH cases has been previously performed2,3,6,10,23. The association of IEGH with craniofacial anomalies, such as cleft palate, implies an origin during early embryogenesis, likely during the 5th to 6th week of gestation, possibly via evagination of a third inferior telencephalic vesicle, in the case of middle cranial fossa lesions24. Patients typically present within the first six months of life, and many are identified via prenatal ultrasonography, although cases in older children have been documented2,3,6,17,24,25. The recommended management for IEGH is staged resections, beginning with the intracranial component3,25. It is important to recognize these lesions as they are benign. Grossly, the lesions are often large and cystic2,3,6,10. Histological examination of previous cases has yielded similar findings as the case presented here; namely, disorganized neuroglial tissue (variably mature neurons, astrocytes, and oligodendrocytes) with scattered calcospherites, and the presence of other CNS tissue elements including leptomeninges, ependyma, choroid plexus, and ocular pigmented epithelium2,3,6,10,11. In some cases, cortical or cerebellar architectural patterns are evident2,10,22. To our knowledge, this is the first example of IEGH with genetic / molecular analysis performed. In contrast to a recent case series of nasal glioma5, this case showed no whole arm chromosomal gains or losses. Overall, the condition appears to have excellent prognosis after resection, including normal neurologic development3,13,25. However, complications related to airway obstruction are possible7,15,16. The infant in this case is doing well at 10 months of age, with normal development and without evidence of growth of the residual oropharyngeal mass. Conflicts of Interest Statement The authors have no conflicts of interest to report. Funding Statement The authors have no relevant funding sources to disclose. References 1 .Zhou JX, Yang X, Ning S, et al. Identification of KANSARL as the first cancer predisposition fusion gene specific to the population of European ancestry origin. Oncotarget. Aug 01 2017;8(31):50594-50607. https://doi.org/10.18632/oncotarget.16385 2 .Oya S, Kawahara N, Aoki S, et al. Intracranial extracerebral glioneuronal heterotopia. Case report and review of the literature. J Neurosurg. Jan 2005;102(1 Suppl):105-12. https://doi.org/10.3171/ped.2005.102.1.0105 3 .Abel TJ, Chowdhary A, Thapa M, et al. Ectopic glioneuronal tissue in the middle cranial fossa region. Report of four cases. J Neurosurg Pediatr. Mar 2009;3(3):188-96. https://doi.org/10.3171/2008.12.PEDS0892 4 .Husein OF, Collins M, Kang DR. Neuroglial heterotopia causing neonatal airway obstruction: presentation, management, and literature review. Eur J Pediatr. Dec 2008;167(12):1351-5. https://doi.org/10.1007/s00431-008-0810-2 5 .Gilani A, Kleinschmidt-DeMasters BK. Histopathologic features of nasal glial heterotopia (nasal glioma). Childs Nerv Syst. Jan 2022;38(1):63-75. https://doi.org/10.1007/s00381-021-05369-4 6 .Gyure KA, Morrison AL, Jones RV. Intracranial extracerebral neuroglial heterotopia: A case report and review of the literature. Ann Diagn Pathol. Jun 1999;3(3):182-6. https://doi.org/10.1016/s1092-9134(99)80047-1 7 .Behar PM, Muller S, Gerber ME, Todd NW. Heterotopic neuroglial tissue causing airway obstruction in the newborn. Arch Otolaryngol Head Neck Surg. Aug 2001;127(8):997-1002. https://doi.org/10.1001/archotol.127.8.997 8 .Knox R, Pratt M, Garvin AJ, White B. Heterotopic lingual brain in the newborn. Arch Otolaryngol Head Neck Surg. May 1989;115(5):630-2. https://doi.org/10.1001/archotol.1989.01860290088021 9 .Barkovich AJ, Guerrini R, Kuzniecky RI, Jackson GD, Dobyns WB. A developmental and genetic classification for malformations of cortical development: update 2012. Brain. May 2012;135(Pt 5):1348-69. https://doi.org/10.1093/brain/aws019 10 .Cho HJ, Kim HN, Kim KJ, et al. Intracranial extracerebral glioneuronal heterotopia with adipose tissue and a glioependymal cyst: a case report and review of the literature. Korean J Pathol. Jun 2014;48(3):254-7. https://doi.org/10.4132/KoreanJPathol.2014.48.3.254 11 .Wakai S, Nakamura K, Arai T, Nagai M. Extracerebral neural tissue mass in the middle cranial fossa extending into the oropharynx in a neonate. Case report. J Neurosurg. Oct 1983;59(4):692-6. https://doi.org/10.3171/jns.1983.59.4.0692 12 .Gallo AE, Smith JD. Intracranial and extracranial neurogenic hamartoma. J Neurosurg. Apr 1977;46(4):517-23. https://doi.org/10.3171/jns.1977.46.4.0517 13 .Misra BK, Shaw JF, Gordon A. Heterotopic brain cyst from middle cranial fossa to submandibular region. Childs Nerv Syst. 1987;3(5):297-300. https://doi.org/10.1007/BF00271828 14 .Moritz JD, Emons D, Wiestler OD, Solymosi L, Kowalewski S, Reiser M. Extracerebral intracranial glioneural hamartoma with extension into the parapharyngeal space. AJNR Am J Neuroradiol. 1995;16(6):1279-81. PMID: 7677025 15 .Nakamura T, Kakinuma H, Imaku M, et al. A large lateral parapharyngeal heterotopic brain tissue extending into the intracranial area. J Child Neurol. Oct 1998;13(10):518-20. https://doi.org/10.1177/088307389801301011 16 .Sinn DP, Wessberg GA, Coln CD, Weinberg AG, Sklar FH. Neonatal asphyxia secondary to Robin complex and neuroglia heterotopia of nasopharynx. Oral Surg Oral Med Oral Pathol. Aug 1981;52(2):137-41. https://doi.org/10.1016/0030-4220(81)90309-1 17 .Ferraz-Filho JR, Torres US, Vaz-Oliani DC, Souza AS. Intracranial extracerebral neuroglial heterotopia with parapharyngeal extension: pre-natal and post-natal imaging findings. Br J Radiol. Feb 2012;85(1010):e41-5. https://doi.org/10.1259/bjr/16277934 18 .Marina MB, Zurin AR, Muhaizan WM, Primuharsa Putra SH, Azizi AB, Kenali MS. Heterotopic neuroglial tissue presenting as oral cavity mass with intracranial extension. Int J Pediatr Otorhinolaryngol. Nov 2005;69(11):1587-90. https://doi.org/10.1016/j.ijporl.2005.04.017 19 .Ball RY, Treip CS. Intracranial extracerebral neuroglial hamartoma. Acta Neuropathol. 1984;65(2):172-6. https://doi.org/10.1007/BF00690474 20 .Farhat SM, Hudson JS. Extracerebral brain heterotopia. Case report. J Neurosurg. Feb 1969;30(2):190-4. https://doi.org/10.3171/jns.1969.30.2.0190 21 .Broniatowski M, Witt WJ, Shah AC, Galloway PG, Abramowsky CR. Glial tissue in the parapharyngeal space. Arch Otolaryngol. Oct 1981;107(10):638-41. https://doi.org/10.1001/archotol.1981.00790460050016 22 .Marubayashi T, Matsukado Y. Intracranial extracerebral brain heterotopia. Case report. J Neurosurg. Mar 1978;48(3):470-4. https://doi.org/10.3171/jns.1978.48.3.0470 23 .Park JE, Park MC, Yoon SH, Kim JH. Intradural extracerebral choristoma. Case report and review of the literature. Pediatr Neurosurg. 2008;44(4):318-23. https://doi.org/10.1159/000134924 24 .Harris CP, Townsend JJ, Klatt EC. Accessory brains (extracerebral heterotopias): unusual prenatal intracranial mass lesions. J Child Neurol. Oct 1994;9(4):386-9. https://doi.org/10.1177/088307389400900410 25 .Muzumdar D, Michaud J, Ventureyra EC. Anterior cranial base glioneuronal heterotopia. Childs Nerv Syst. Mar 2006;22(3):227-33. https://doi.org/10.1007/s00381-005-1222-5
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |