|
|
|
Free Neuropathology 5:27 (2024) |
|
Case Report |
|
Regression of multiple intracranial meningiomas after cessation of long-term synthetic progesterone (megestrol) medication: case report and autopsy |
|
Tamadar A. AlDoheyan1,2, Marc R. Del Bigio1,3 |
|
|
Corresponding author: |
|
Submitted: 16 August 2024 |
|
Keywords: Autopsy, Meningioma, Megestrol, Progesterone receptor, Tumor involution |
|
Abstract We report the history of a woman who developed four intracranial meningiomas during 11 years of therapy with the synthetic progesterone agonist megestrol. After discontinuation of the drug at age 75 years, she improved clinically and a CT scan showed near complete regression of the meningiomas by 78 years. Autopsy was performed at 83 years of age following an accidental death. At the tumor sites, we found both collagenous tissue with small islands of low grade meningioma having strong nuclear immunoreactivity for progesterone receptor and lipomatous tissue. A literature review showed similar cases of radiologic meningioma regression following discontinuance of progestins. Our case is the first one with histopathologic characterization of the end point. |
|
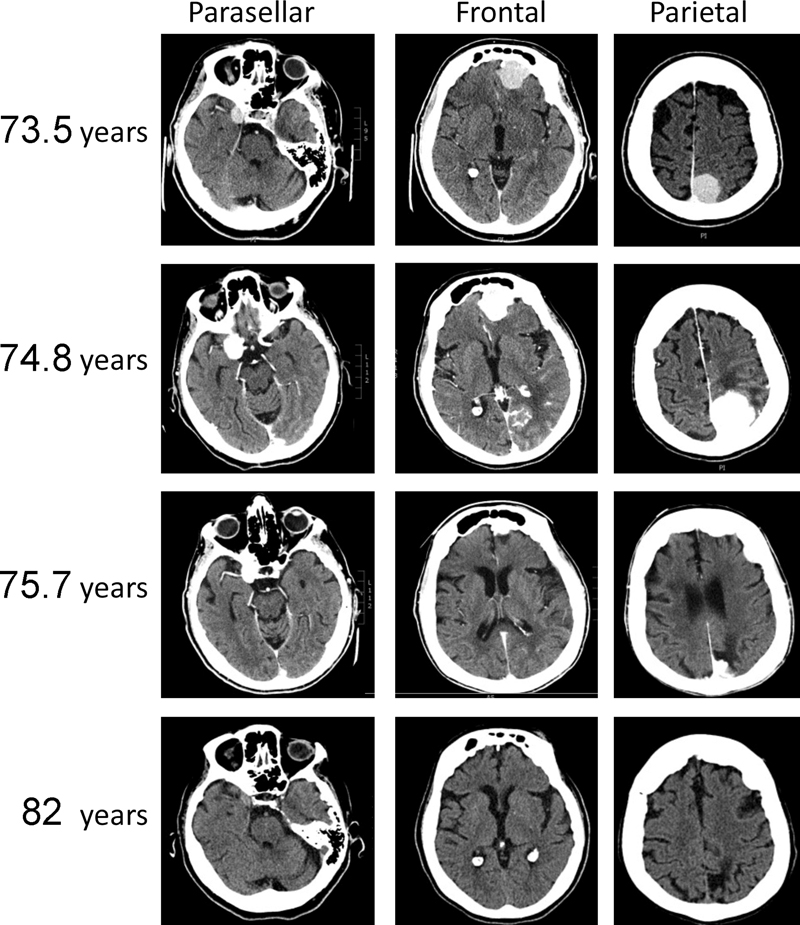
Introduction Meningiomas are twice as common in females as in males. These tumors are known to express progesterone receptor and to a lesser extent estrogen receptors [1, 2]. Numerous case reports and population-based studies show increased risk for meningioma, tumor multiplicity, and tumor progression in women who receive synthetic progestins including cyproterone acetate, megestrol acetate (also called nomegestrol), and chlormadinone acetate [3–10]. Progestin-associated meningiomas are often located at the skull base and have higher frequencies of PIK3CA and TRAF7 mutations [11]. Some tumors decrease in size after drug discontinuation [12, 13], although administration of the antiprogesterone agent mifepristone has not been shown to be efficacious for treatment of progestin-induced meningioma [14, 15]. Here we report the autopsy findings in a woman who developed multiple intracranial tumors during long-term therapy with the progesterone agonist megestrol acetate. The tumors, presumed to be meningiomas, regressed almost entirely upon cessation of the drug. Clinical summary At 64 years age, this woman underwent hysterectomy with bilateral salpingo-oophorectomy for low grade endometrial stromal sarcoma and was placed on progesterone therapy with megestrol 160 mg daily. Regular imaging follow-up in the subsequent decade showed no evidence of local recurrence or metastatic disease. Psoriasis had been treated with oral methotrexate intermittently from age 62 to 73 years, acitretin, a retinoid, for 1 year at age 74, and apremilast, a selective inhibitor of the enzyme phosphodiesterase 4 / PDE4, from age 77 to 83. The past medical history of the woman also included diabetes mellitus type 2, hypothyroidism, and arterial hypertension for which she was treated with metformin, levothyroxine, nifedipine, and hydrochlorothiazide, respectively. CT scans of the head had been done at 56 and 66 years because of headaches; these showed minor ischemic changes in cerebral white matter and no evidence of intracranial tumor. At age 73 years, the woman presented with labile emotions and confusion. She had a mild resting tremor but no localizing signs. A CT scan of the head showed three dura-based tumors in the left parietal / posterior falx region (2.9 cm), the left frontal / anterior falx region (2.8 cm), and the right parasellar region (1.7 cm) (Figures 1 and 2). Measurements presented in Figure 2 are from the CT scans. All tumors were isointense with gray matter on unenhanced imaging, and all were bright following contrast enhancement. The tumors were thought to be meningiomas. A single magnetic resonance (MR) study was incomplete because of claustrophobia. The brain tumors were isointense on the T1 sequence. Approximately 1 year later at 74.8 years of age, the woman stopped eating and was unable to walk, whereupon she was admitted to hospital. A CT scan at the time of admission showed further enlargement of two tumors with significant local mass effect and surrounding vasogenic edema (Figure 1). The woman was judged not to be a candidate for neurosurgical intervention. A CT scan two months after discontinuation of megestrol showed that the two largest tumors had decreased in size, whereas a new small en plaque tumor had appeared in the lateral part of the left frontal lobe. During a one year hospital stay without specific anti-neoplastic therapy, the neurologic status of the woman gradually improved. A CT scan at 75.7 years age showed that all tumors had decreased (Figure 1 and Figure 2). At age 76 years, the woman returned to independent living and regained her motor vehicle driving license. At age 77 years her tremor had increased slightly. CT scans at 78 and 82 years age showed mild diffuse cerebral atrophy and all intracranial tumors had disappeared by 82 years age (Figure 1 and Figure 2). The woman died after choking on food at 83 years.
Figure 1. CT scans with contrast enhancement of brain showing dura-based tumors in the right parasellar, left frontal, and left parietal regions in a woman at ages 73.5 and 74.8 years when taking megestrol, and at ages 75.7 years and 82 years, after megestrol had been discontinued.
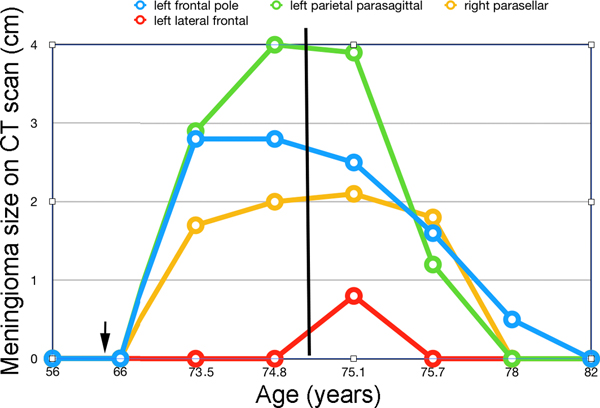
Figure 2. Line graph showing change in meningioma sizes on CT scans over time. Tumor size (in cm) is reported for the greatest dimension only. The arrow shows the time when megestrol was started and the vertical line shows the time when megestrol was discontinued. Complete autopsy was performed 3 days after death. The body was that of a thin female with no somatic evidence of malignancy, including in the pelvis at the site of the original endometrial sarcoma. Pathological findings The brain weight was 1137 g. The inner surface of the skull had extensive lobulated hyperostotic areas involving both frontal bones. Corresponding to the sites of the tumors identified on earlier CT scans, the dura mater along the skull base anterior to the left olfactory groove had a soft, yellow lesion (approximately 2 x 1 x < 0.3 cm) (Figure 3a). The dura mater in the right parasellar region was thickened and yellow. The internal surface of the paramedian left parietal convexity dura was focally thickened (approximately 3 x 2 x 0.5 cm) with adhesion to the brain (Figure 3b). The leptomeninges were unremarkable. Coronal slices through the cerebral hemispheres demonstrated minimal focal atrophy in the left frontal lobe tip and more pronounced atrophy with cavitation of the subcortical white matter in the left medial parietal region.
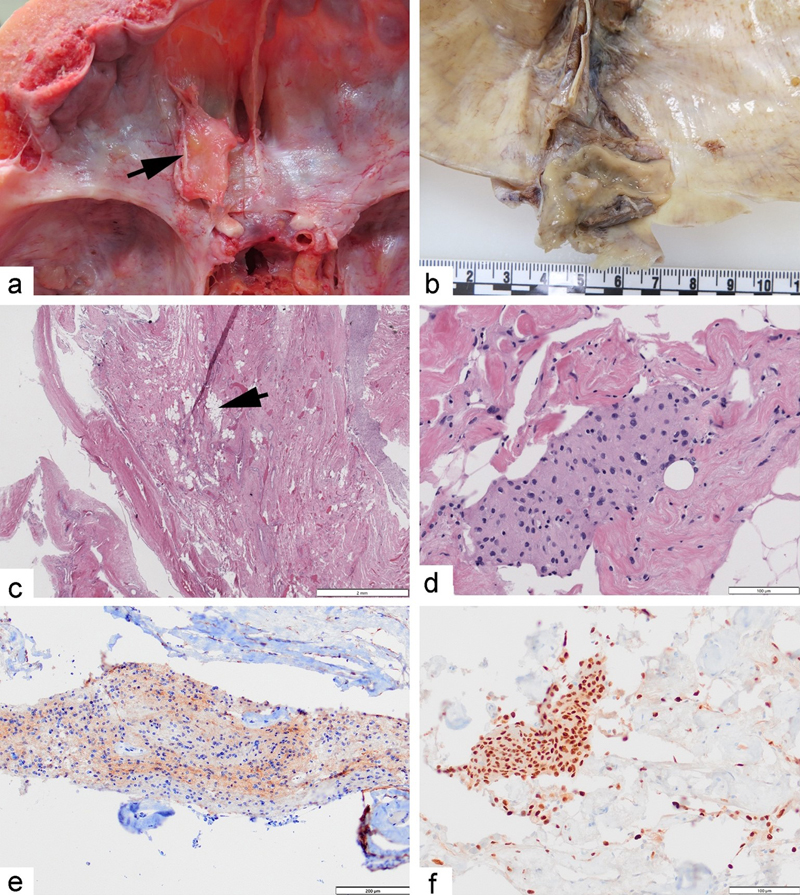
Figure 3. a) Photograph showing the anterior cranial fossa with left frontal bone hyperostosis and yellowish thick, firm tissue (arrow) reflected from the anterior falx cerebri at the time of autopsy. b) Photograph showing the thickened dura mater near the superior sagittal sinus in the left parietal region after formalin fixation. c) Photomicrograph showing the left parietal dura and fibrotic tumor with lipomatous meningioma (arrow). Hematoxylin & eosin stain, original magnification 12.5x. d) Photomicrograph showing a cluster of meningothelial cells in the left frontal tumor. H&E stain, original magnification 200x. e) Photomicrograph showing the residual left parietal tumor with immunoreactivity for epithelial membrane antigen (EMA) in brown with blue hematoxylin counterstain. Original magnification 100x. f) Photomicrograph showing the residual left frontal tumor with nuclear immunoreactivity for progesterone receptor (PR) in brown. Original magnification 200x. Microscopic features of the dura mater from the three identifiable previous tumor sites were all similar showing multiple small collections of meningothelial cells (Figure 3d), fibrovascular hyperplasia, and focal lipomatous meningioma (Figure 3c). The latter resembled adipose tissue and did not include meningothelial cells with foamy cytoplasm i.e. lipidized or xanthomatous change [16, 17]. Immunostains for epithelial membrane antigen (EMA) and progesterone receptor (PR) highlighted the meningothelial cell aggregates buried within the collagenous tissue (Figures 3e and 3f). Nuclei in the lipomatous component were predominantly negative for PR. The cells were negative for cytokeratin (AE1AE3), estrogen receptor (ER), WT1, and CD10 although fibroblasts and lipomatous cells were positive for CD10. This excludes the remote possibility that these lesions represented metastatic endometrial stromal sarcoma. An immunostain for Ki67 showed no cell proliferation in the meningothelial aggregates. Based upon the histopathological features, we conclude that these lesions represent regressed meningiomas. Based upon the history of regression, inflammatory pseudotumor was also considered, but the patient had been on no anti-inflammatory therapy and the residual tissue mass showed no features of inflammation. A small focus of extramedullary hematopoiesis was present in the parasellar region. The left frontal lobe tip and the left medial occipital parietal region at the sites of the previous tumors were atrophic. In addition to the intracranial tumors, there was an intermediate level of Alzheimer disease type neuropathologic change (NIA-AA score A2, B2, C2) [18] and there were extremely rare cortical Lewy bodies. There was no evidence for brainstem neurodegenerative changes to explain her tremor or swallowing difficulty. Discussion Spontaneous regression of intracranial meningiomas is rare and the histopathology of regressed meningiomas is not well documented. In this case report, we describe a woman with multiple meningiomas that appeared after a seven year period of treatment with megestrol, a synthetic progesterone, and that vanished approximately three years after discontinuation of the drug. It has been reported that meningiomas rarely regress following administration of estrogen antagonists e.g. mepitiostane [19], post-partum [20], following menopause [21], or “spontaneously” [22]. Several case reports and small series show radiologic regression of meningiomas after cessation of progestin therapies with chlormadinone acetate, megestrol acetate, and cyproterone acetate [23–29]. In one series, osseous hypertrophy at the sites of regressed tumors was documented [8]. Notably, tumor growth and regression could not be attributed temporally to any other medication or disease process. Recent reviews of biological therapies used for dermatologic diseases including psoriasis highlighted very rare cases in which meningiomas were diagnosed in patients receiving methotrexate, secukinumab or etanercept. The authors concluded that these drugs did not appear to cause, exacerbate, or shrink the tumors [30, 31]. One woman was prescribed apremilast, an inhibitor of phosphodiesterase 4 (PDE4), for her psoriasis during the period of meningioma regression [32]. Although PDE4 is reported to be expressed in some meningiomas, there is no evidence that PDE4 inhibition can treat meningiomas [33]. In our case, the residual meningothelial cells were strongly immunoreactive for progesterone receptor (PR), as is often reported for meningioma [1]. In cell culture, the presence of PR determines the responsiveness of meningothelial cells to progesterone [34]. Other experiments showed that progesterone in the culture medium does not have direct mitogenic effects but increases the sensitivity of meningioma cells to other mitogenic stimuli [35]. Specific molecular effects of the synthetic progesterone agonist megestrol have not been studied in detail in meningioma cells. Seemingly paradoxically, megestrol inhibits proliferation of cultured breast cells that express PR [36]. Meningiomas however differentially express several distinct steroid receptor coactivators [37], which might explain why their response to sex hormones is variable and unpredictable [38]. The present report is the first one to show the histopathologic endpoint associated with meningioma regression. Small clusters of residual meningothelial tumor cells were present in a background of lipomatous tissue. The lipomatous variant of meningioma is a rare but well-recognized entity [16]. It should be noted that the tumors, at their apex, had specific imaging characteristics with isointensegray matter on CT and MR suggestive of more common forms of meningioma, in contrast to the features of lipomatous meningioma which are hypointense on CT scans and hyperintense on T1-weighted MR [39]. Whether conversion of meningioma to lipomatous meningioma [16] necessarily accompanies regression is unknown. Some authors have argued about the nature of this is phenomenon which may be regressive or metaplastic [16, 39, 40]. Conflicts of Interest Statement The authors have no conflicts of interest to report. Funding Statement The authors acknowledge that they received no funding in support for this work. Informed consent Permission to publish this report was explicitly granted by the next of kin. The University of Manitoba Research Ethics and Compliance committee approved the case report (reference # HS25528). References 1. Maiuri F, Mariniello G, de Divitiis O, et al. (2021) Progesterone receptor expression in meningiomas: pathological and prognostic implications. Frontiers in oncology 11: 611218. https://doi.org/10.3389/fonc.2021.611218 2. Telugu RB, Chowhan AK, Rukmangadha N, et al. (2020) Estrogen and progesterone receptor in meningiomas: An immunohistochemical analysis. J Cancer Res Ther 16(6): 1482-1487. https://doi.org/10.4103/jcrt.JCRT_1075_16 3. Harland TA, Freeman JL, Davern M, et al. (2018) Progesterone-only contraception is associated with a shorter progression-free survival in premenopausal women with WHO Grade I meningioma. J Neurooncol 136(2): 327-333. https://doi.org/10.1007/s11060-017-2656-9 4. Graillon T, Boissonneau S, Appay R, et al. (2021) Meningiomas in patients with long-term exposition to progestins: Characteristics and outcome. Neuro-Chirurgie 67(6): 556-563. https://doi.org/10.1016/j.neuchi.2021.04.018 5. Hoisnard L, Laanani M, Passeri T, et al. (2022) Risk of intracranial meningioma with three potent progestogens: a population-based case-control study. Eur J Neurol in press. https://doi.org/10.1111/ene.15423 6. Samarut E, Lugat A, Amelot A, et al. (2021) Meningiomas and cyproterone acetate: a retrospective, monocentric cohort of 388 patients treated by surgery or radiotherapy for intracranial meningioma. J Neurooncol 152(1): 115-123. https://doi.org/10.1007/s11060-020-03683-6 7. Nguyen P, Roland N, Neumann A, et al. (2024) Prolonged use of nomegestrol acetate and risk of intracranial meningioma: a population-based cohort study. Lancet Reg Health Eur 42: 100928. https://doi.org/10.1016/j.lanepe.2024.100928 8. Florea SM, Passeri T, Abbritti R, et al. (2023) Opposed evolution of the osseous and soft parts of progestin-associated osteomeningioma after progestin intake discontinuation. Journal of neurosurgery 139(4): 944-952. https://doi.org/10.3171/2022.12.JNS222006 9. Roland N, Neumann A, Hoisnard L, et al. (2024) Use of progestogens and the risk of intracranial meningioma: national case-control study. BMJ (Clinical research ed) 384: e078078. https://doi.org/10.1136/bmj-2023-078078 10. Raj R, Korja M, Koroknay-Pál P, Niemelä M (2018) Multiple meningiomas in two male-to-female transsexual patients with hormone replacement therapy: A report of two cases and a brief literature review. Surg Neurol Int 9: 109. https://doi.org/10.4103/sni.sni_22_18 11. Peyre M, Gaillard S, de Marcellus C, et al. (2018) Progestin-associated shift of meningioma mutational landscape. Ann Oncol 29(3): 681-686. https://doi.org/10.1093/annonc/mdx763 12. Samoyeau T, Provost C, Roux A, et al. (2022) Meningioma in patients exposed to progestin drugs: results from a real-life screening program. J Neurooncol 160(1): 127-136. https://doi.org/10.1007/s11060-022-04124-2 13. Passeri T, Giammattei L, Le Van T, et al. (2022) Atypical evolution of meningiomatosis after discontinuation of cyproterone acetate: clinical cases and histomolecular characterization. Acta Neurochir (Wien) 164(1): 255-263. https://doi.org/10.1007/s00701-021-05005-9 14. AbiJaoude S, Marijon P, Roblot P, et al. (2021) Sustained growth of intraosseous hormone-associated meningiomas after cessation of progestin therapy. Acta Neurochir 163(6): 1705-1710. https://doi.org/10.1007/s00701-021-04781-8 15. Ji Y, Rankin C, Grunberg S, et al. (2015) Double-blind phase III randomized trial of the antiprogestin agent mifepristone in the treatment of unresectable meningioma: SWOG S9005. J Clin Oncol 33(34): 4093-4098. https://doi.org/10.1200/JCO.2015.61.6490 16. Roncaroli F, Scheithauer BW, Laeng RH, Cenacchi G, Abell-Aleff P, Moschopulos M (2001) Lipomatous meningioma: a clinicopathologic study of 18 cases with special reference to the issue of metaplasia. Am J Surg Pathol 25(6): 769-775. https://doi.org/10.1097/00000478-200106000-00008 17. Wong YP, Tan GC, Kumar R (2018) Xanthomatous meningioma: A metaplastic or degenerative phenomenon? Neuropathology : official journal of the Japanese Society of Neuropathology 38(6): 619-623. https://doi.org/10.1111/neup.12511 18. Montine TJ, Phelps CH, Beach TG, et al. (2012) National Institute on Aging-Alzheimer's Association guidelines for the neuropathologic assessment of Alzheimer's disease: a practical approach. Acta Neuropathol 123(1): 1-11. https://doi.org/10.1007/s00401-011-0910-3 19. Oura S, Sakurai T, Yoshimura G, et al. (2000) Regression of a presumed meningioma with the antiestrogen agent mepitiostane. Case report. Journal of neurosurgery 93(1): 132-135. https://doi.org/10.3171/jns.2000.93.1.0132 20. Chakravarthy V, Kaplan B, Gospodarev V, Myers H, De Los Reyes K, Achiriloaie A (2018) Houdini tumor: case report and literature review of pregnancy-associated meningioma. World neurosurgery 114: e1261-e1265. https://doi.org/10.1016/j.wneu.2018.03.187 21. Takada M, Yanaka K, Nakamura K, Akimoto K, Takeda H, Ishikawa E (2022) Spontaneous regression of a posterior fossa meningioma: A case report. Surg Neurol Int 13: 334. https://doi.org/10.25259/SNI_429_2022 22. Hirota K, Fujita T, Akagawa H, Onda H, Kasuya H (2014) Spontaneous regression together with increased calcification of incidental meningioma. Surg Neurol Int 5: 73. https://doi.org/10.4103/2152-7806.132957 23. Shimizu J, Matsumoto M, Yamazaki E, Yasue M (2008) Spontaneous regression of an asymptomatic meningioma associated with discontinuation of progesterone agonist administration. Neurol Med Chir 48(5): 227-230. https://doi.org/10.2176/nmc.48.227 24. Vadivelu S, Sharer L, Schulder M (2010) Regression of multiple intracranial meningiomas after cessation of long-term progesterone agonist therapy. J Neurosurg 112(5): 920-924. https://doi.org/10.3171/2009.8.JNS09201 25. Bernat AL, Oyama K, Hamdi S, et al. (2015) Growth stabilization and regression of meningiomas after discontinuation of cyproterone acetate: a case series of 12 patients. Acta Neurochir 157(10): 1741-1746. https://doi.org/10.1007/s00701-015-2532-3 26. Goncalves AM, Page P, Domigo V, Meder JF, Oppenheim C (2010) Abrupt regression of a meningioma after discontinuation of cyproterone treatment. AJNR American journal of neuroradiology 31(8): 1504-1505. https://doi.org/10.3174/ajnr.A1978 27. Cebula H, Pham TQ, Boyer P, Froelich S (2010) Regression of meningiomas after discontinuation of cyproterone acetate in a transsexual patient. Acta Neurochir 152(11): 1955-1956. https://doi.org/10.1007/s00701-010-0787-2 28. Voormolen EHJ, Champagne PO, Roca E, et al. (2021) Intracranial meningiomas decrease in volume on magnetic resonance imaging after discontinuing progestin. Neurosurgery 89(2): 308-314. https://doi.org/10.1093/neuros/nyab175 29. Bernat AL, Bonnin S, Labidi M, et al. (2018) Regression of giant olfactory groove meningioma and complete visual acuity recovery after discontinuation of cyproterone acetate. J Ophthalmic Vis Res 13(3): 355-358. https://doi.org/10.4103/jovr.jovr_21_17 30. Mastorino L, Dapavo P, Avallone G, et al. (2022) Biologic treatment for psoriasis in cancer patients: should they still be considered forbidden? J Dermatolog Treat 33(5): 2495-2502. https://doi.org/10.1080/09546634.2021.1970706 31. Finnegan P, Ahmad K, Sadlier M, Lynch M (2023) A retrospective review of the management of patients following a malignancy diagnosis on biologic therapies for the treatment of dermatological disorders. JAAD Case Rep 39: 81-87. https://doi.org/10.1016/j.jdcr.2023.07.007 32. Schick MA, Schlegel N (2022) Clinical implication of phosphodiesterase-4-inhibition. International journal of molecular sciences 23(3): 1209. https://doi.org/10.3390/ijms23031209 33. Goldhoff P, Warrington NM, Limbrick DD, Jr., et al. (2008) Targeted inhibition of cyclic AMP phosphodiesterase-4 promotes brain tumor regression. Clin Cancer Res 14(23): 7717-7725. https://doi.org/10.1158/1078-0432.CCR-08-0827 34. Carroll RS, Zhang J, Dashner K, Black PM (1995) Progesterone and glucocorticoid receptor activation in meningiomas. Neurosurgery 37(1): 92-97. https://doi.org/10.1227/00006123-199507000-00014 35. Koper JW, Lamberts SW (1994) Meningiomas, epidermal growth factor and progesterone. Hum Reprod 9 Suppl 1: 190-194. https://doi.org/10.1093/humrep/9.suppl_1.190 36. Botella J, Duranti E, Duc I, Cognet AM, Delansorne R, Paris J (1994) Inhibition by nomegestrol acetate and other synthetic progestins on proliferation and progesterone receptor content of T47-D human breast cancer cells. J Steroid Biochem Mol Biol 50(1-2): 41-47. https://doi.org/10.1016/0960-0760(94)90170-8 37. Carroll RS, Brown M, Zhang J, DiRenzo J, Font De Mora J, Black PM (2000) Expression of a subset of steroid receptor cofactors is associated with progesterone receptor expression in meningiomas. Clin Cancer Res 6(9): 3570-3575. PMID: 10999746 38. Agopiantz M, Carnot M, Denis C, Martin E, Gauchotte G (2023) Hormone receptor expression in meningiomas: a systematic review. Cancers 15(3): 980. https://doi.org/10.3390/cancers15030980 39. Lapolla P, Familiari P, Zancana G, et al. (2021) Lipomatous meningioma: clinical-pathological findings, imaging characterisation and correlations of a rare type of meningioma. In Vivo 35(6): 3031-3037. https://doi.org/10.21873/invivo.12598 40. Bolat F, Kayaselcuk F, Aydin MV, Erdogan B, Ulusan S, Zorludemir S (2003) Lipidized or lipomatous meningioma, which is more appropriate? A case report. Neurol Res 25(7): 764-766. https://doi.org/10.1179/016164103101202147
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |