|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Free Neuropathology 5:6 (2024) |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Letter |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Searching for a cut-off point for p53 immunohistochemistry as evidence of TP53 mutations |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Ilay Caliskan1, Rufei Lu1, Cristine Szu Lyn Ding1,2, Francineide Sadala de Souza1,3, Arie Perry1, Tarik Tihan1 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Corresponding author: |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Submitted: 23 January 2024 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Keywords: p53, Immunohistochemistry, TP53 mutation, Glioma |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Numerous publications and revised grading strategies reiterate the relevance of TP53 gene mutations for adult diffuse gliomas1–3. These studies identify TP53 mutation as a frequent alteration in IDH-mutant astrocytomas along with other critical genes, such as IDH1, IDH2, and ATRX. The 2021 WHO classification of Central Nervous System (CNS)4 designates "strong" nuclear expression of p53 protein in greater than 10 % of tumor cells, which implies the presence of TP53 mutations4 as a desirable criterion for IDH-mutant astrocytomas. Other studies have also recognized similar percentages in adult diffuse gliomas as evidence of TP53 mutations. To incorporate TP53 alterations into the diagnostic work-up, these studies used immunohistochemistry as a viable alternative to provide the type and grade of diffuse astrocytomas5, and others recommended p53 protein immunohistochemistry as a reliable means of predicting TP53 mutations6,7,8. While a few studies report an association with treatment response, most studies do not find TP53 mutation status or positive immunohistochemical staining helpful in determining biological behavior or type of adult diffuse glioma8. Contrary to the studies that expressed enthusiasm for p53 immunohistochemistry as a predictive marker for TP53 mutational status7, studies as far back as 25 years ago pointed to the discordance between p53 protein expression and TP53 mutations9. It was clear from these earlier studies that most gliomas with focal p53 nuclear immunopositivity do not harbor TP53 mutations9. Certain alterations in the TP53 gene, such as exon 4 mutations or missense mutations, are more likely to lead to strong positive staining10, while truncating mutations (e.g., nonsense, splice site, or frameshift) are associated with absence or barely detectable p53 protein immunopositivity ("null phenotype")11. Even among the few studies that propose p53 staining as a practical prognostic marker, there is little agreement on the optimal cut-off value. Some studies presuming TP53 mutations based on p53 immunostaining simply used "positive" staining while others did not report definitions for p53 positivity, further confounding the literature11–13. One of the most recent comparative studies claimed 10 % positivity as a cut-off point to predict TP53 mutation based on receiver operating characteristic curve (ROC) analysis12, quoted by the WHO 2021 classification4. To determine a practical value for p53 immunostaining in everyday neuropathology practice and to validate whether a 10 % cut-off can be reliably used to suggest TP53 mutation (as suggested by WHO 2021), we analyzed a group of diffuse gliomas for p53 staining and TP53 mutations. We identified all adult diffuse gliomas and diffuse midline gliomas for which analysis of p53 immunohistochemistry and TP53 mutation was performed during a five-year period. The inclusion criteria were: 1) diagnosis of adult diffuse glioma or diffuse midline glioma between 2015 and 2020, 2) available p53 (DO-7 clone) immunohistochemistry staining, and 3) available analysis with next generation sequence analysis (NGS), referred to as "UCSF500 NGS" panel14, which includes a comprehensive assessment of all TP53 coding exons and most other genes known to be recurrently altered in CNS tumors15. Clinical and radiological features were obtained from electronic patient records. All cases were re-analyzed for p53 protein labeling index (LI) to ensure uniform assessment based on strong nuclear staining (equal to or greater than the intensity of positive control tissue) of p53 protein in tumor cells (Figure 1). The positive control tissue was validated by UCSF500 NGS for TP53 mutation at the UCSF Histology and Clinical Cancer Genomics Laboratory. The p53 LIs were determined by the available original reported LI, which was achieved by capturing a digital image of the area with highest labeling and counting at least 500 cells in the captured image, followed by the re-assessment of the image by two of the authors independently to estimate the LI within a 5 % maximum variance. Genetic alterations involving the tumor and germline were determined as previously described15,16. Statistical analyses were performed using R version 4.2.2. A receiver operator characteristic curve (ROC) was analyzed using cutpointr R package (version 1.1.1). Violin plot and pie chart were generated using ggplot2 R package (version 3.3.5). The study was approved by UCSF Committee for Human Research (UCSF CHR 10-01252).
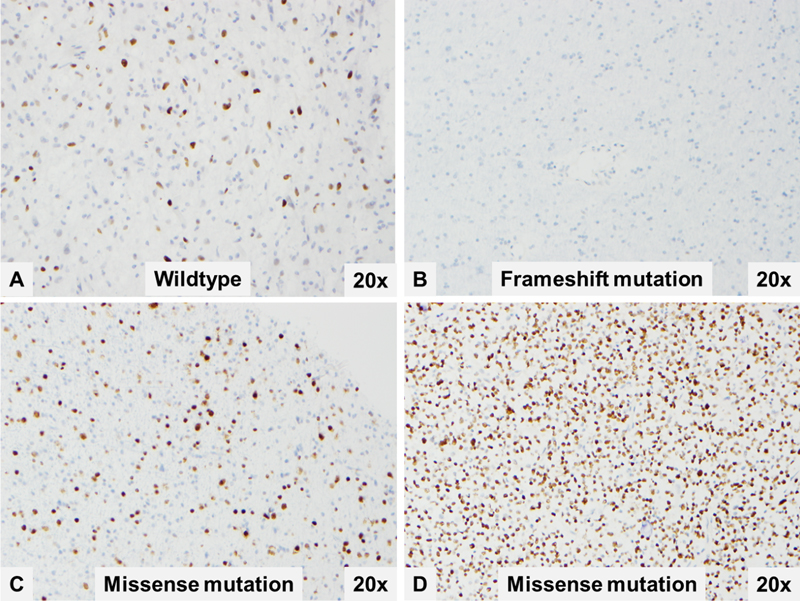
Figure 1. Representative p53 immunostaining patterns that were molecularly confirmed as TP53 wildtype (A), TP53 frameshift mutation (B) and TP53 missense mutations (C and D). Our study group was composed of 99 patients with an average age of 44.5 years (range 1-81 years). There were 49 female and 50 male patients. Tumor types and locations are presented in Table 1. Seventy-six (76) of the samples were from primary tumors (first resection) while 23 were from recurrent tumors. Two glioblastomas had earlier biopsies at another hospital without additional treatment before the patient was transferred to our institution. Seventy-two (72) of the primary tumors were CNS WHO grade 4, six were CNS WHO grade 3, and twenty-one tumors were CNS WHO grade 2. There were 52 TP53-mutant and 47 TP53-wildtype tumors and the distribution of these mutations among tumor types is presented in Table 1. Forty-two (42) tumors had missense mutations, while three others had missense combined with frameshift mutations. There were 3 tumors with frameshift mutation-only (Figure 2B). Table 1. Demographics, location of tumor, and final diagnosis
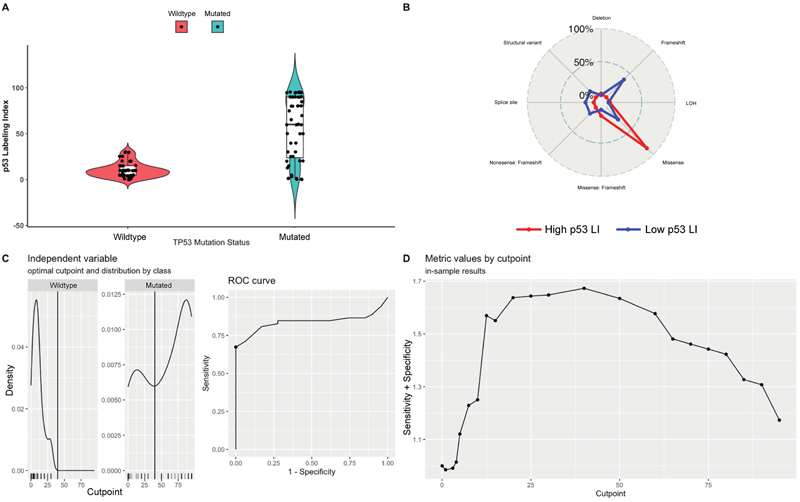
The median p53 immunohistochemistry labeling index for tumors harboring TP53 mutation was 60 % (Range: 0-95 %) with an interquartile range (IQR) of 66.25 %, while the median value for those without TP53 mutations was 10 % with an IQR of 10.5 % (Range: 0-30 %). When 42 tumors with missense mutations were considered, the median labeling index was calculated as 77.5 % (mean 64.24 %), and the median labeling index for cases with frameshift mutations was 12.5 % (mean 21 %). However, there was a wide range of labeling indices for missense (1-95 %) mutations. Of note, out of 11 tumors with absent p53 staining, 6 had TP53 mutations (two frameshift, two missense, one splice site mutation, and one structural variant).
Figure 2. Labeling index of p53 is significantly higher in TP53-mutated group as shown in the violin plot (A). Radar chart for TP53 mutation types in tumor with high p53 LI (>40 %) and low p53 (<1 %) LI (B). ROC analysis demonstrated 40 % as an optimal cutoff point for TP53 mutation based on UCSF500 NGS confirmation (C and D). (LOH: Loss of heterozygosity, Cutpoint: mean value of the optimal cutoff, Density: distribution of cutoff values). When the cut-off values for p53 immunohistochemistry were considered, the positive predictive value of 10 % labeling index was calculated as 60.4 %, while the negative predictive value at the same cut-off point was 70.6 %. An ROC analysis based on the 99 patients demonstrated that strong p53 staining in more than 40 % of tumor cells provided the most accurate prediction of mutation based on Youden index (Figure 2). Using this cutoff value, positive predictive value (PPV), negative predictive value (NPV), sensitivity, and specificity were 100 %, 73.6 %, 67 %, and 100 %, respectively. Most of the inaccuracy could be attributed to tumors with frameshift mutations, which frequently demonstrated the null cell pattern with absent immunostaining (with p53 LI of <1 %). After excluding the tumor with frameshift mutations, an ROC analysis redemonstrated that the best cutoff for p53 LI as still 40 % with PPV, NPV, sensitivity, and specificity calculated as 100 %, 81 %, 88 %, and 100 %, respectively. These findings suggest, as previously demonstrated by many, that p53 immunostaining cannot be taken as prima facia evidence of TP53 mutations. Furthermore, our data suggest that the cut-off value recommended by the CNS WHO classification to predict TP53 mutations may be inaccurate and should be reevaluated. This issue underscores the problem of accepting results of single studies without appropriate validation and confirmation by more than one independent scientific observation for the purposes of standardized classification systems that would be used worldwide. We believe that previously suggested p53 labeling index of 10 % as predictive of TP53 mutation significantly overestimates mutations, which could potentially lead to erroneous conclusions in the absence of molecular confirmation. Considering possible variations when performed in different laboratories and using different antibodies, this cut-off value becomes even less predictive. For practical purposes, we recommend the use of >40 % as a more robust and predictive cut-off value for p53 immunohistochemistry, while still acknowledging that there will always be outliers regardless of the cut-off number utilized. Finally, the absence of staining does not rule out a TP53 mutation, and thus should be interpreted with caution. References 1. Appin CL, Brat DJ. Biomarker-driven diagnosis of diffuse gliomas. Mol Aspects Med [Internet] 2015 [cited 2023 Mar 4];45:87–96. https://doi.org/10.1016/j.mam.2015.05.002 2. DJ B, RG V, KD A, et al. Comprehensive, Integrative Genomic Analysis of Diffuse Lower-Grade Gliomas. N Engl J Med [Internet] 2015 [cited 2023 Mar 4];372(26):2481–98. https://doi.org/10.1056/nejmoa1402121 3. Eckel-Passow JE, Lachance DH, Molinaro AM, et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors. New England Journal of Medicine [Internet] 2015 [cited 2023 Mar 4];372(26):2499–508. https://doi.org/10.1056/NEJMoa1407279 4. Brat DJ, Reuss DE, von Deimling A, et al. WHO Classification of Tumours Editorial Board. Central nervous system tumours. 5th ed. 2021. 5. Takano S, Ishikawa E, Sakamoto N, et al. Immunohistochemistry on IDH 1/2, ATRX, p53 and Ki-67 substitute molecular genetic testing and predict patient prognosis in grade III adult diffuse gliomas. Brain Tumor Pathol [Internet] 2016 [cited 2023 Mar 4];33(2):107–16. https://doi.org/10.1007/s10014-016-0260-x 6. Ogura R, Tsukamoto Y, Natsumeda M, et al. Immunohistochemical profiles of IDH1, MGMT and P53: practical significance for prognostication of patients with diffuse gliomas. Neuropathology [Internet] 2015 [cited 2023 Mar 4];35(4):324–35. https://doi.org/10.1111/neup.12196 7. Shao LW, Pan Y, Qi XL, et al. ATRX loss in adult supratentorial diffuse astrocytomas correlates with p53 over expression and IDH1 mutation and predicts better outcome in p53 accumulated patients. Histol Histopathol [Internet] 2016 [cited 2023 Mar 4];31(1):103–14. https://doi.org/10.14670/hh-11-664 8. Antonelli M, Buttarelli FR, Arcella A, et al. Prognostic significance of histological grading, p53 status, YKL-40 expression, and IDH1 mutations in pediatric high-grade gliomas. J Neurooncol [Internet] 2010 [cited 2023 Mar 4];99(2):209–15. https://doi.org/10.1007/s11060-010-0129-5 9. Newcomb EW, Madonia WJ, Pisharody S, Lang FF, Koslow M, Miller DC. A correlative study of p53 protein alteration and p53 gene mutation in glioblastoma multiforme. Brain Pathol [Internet] 1993 [cited 2023 Mar 4];3(3):229–35. https://doi.org/10.1111/j.1750-3639.1993.tb00749.x 10. Faria MHG, Neves Filho EHC, Alves MKS, Burbano RMR, de Moraes Filho MO, Rabenhorst SHB. TP53 mutations in astrocytic gliomas: an association with histological grade, TP53 codon 72 polymorphism and p53 expression. APMIS [Internet] 2012 [cited 2023 Mar 4];120(11):882–9. https://doi.org/10.1111/j.1600-0463.2012.02918.x 11. Gillet E, Alentorn A, Doukouré B, et al. TP53 and p53 statuses and their clinical impact in diffuse low grade gliomas. J Neurooncol [Internet] 2014 [cited 2023 Mar 4];118(1):131–9. https://doi.org/10.1007/s11060-014-1407-4 12. Takami H, Yoshida A, Fukushima S, et al. Revisiting TP53 Mutations and Immunohistochemistry-A Comparative Study in 157 Diffuse Gliomas. Brain Pathol [Internet] 2015 [cited 2023 Mar 4];25(3):256–65. https://doi.org/10.1111/bpa.12173 13. Oka H, Utsuki S, Tanizaki Y, et al. Clinicopathological features of human brainstem gliomas. Brain Tumor Pathol [Internet] 2013 [cited 2023 Mar 4];30(1):1–7. https://doi.org/10.1007/s10014-012-0099-8 14. Lucas CHG, Solomon DA, Perry A. A review of recently described genetic alterations in central nervous system tumors. Hum Pathol [Internet] 2020 [cited 2023 Mar 4];96:56–66. https://doi.org/10.1016/j.humpath.2019.10.009 15. Chenn A, Parker S, Degeare SP, et al. PATH-05. IMPLEMENTATION OF A TARGETED NEXT-GENERATION SEQUENCING PANEL FOR THE DIAGNOSIS AND PRECISION MEDICINE TREATMENT OF ADULT PATIENTS WITH WHO GRADE IV DIFFUSE GLIOMAS. Neuro Oncol [Internet] 2018 [cited 2023 Mar 4];20(suppl_6):vi158–9. https://doi.org/10.1093/neuonc/noy148.661 16. Kline CN, Joseph NM, Grenert JP, et al. Targeted next-generation sequencing of pediatric neuro-oncology patients improves diagnosis, identifies pathogenic germline mutations, and directs targeted therapy. Neuro Oncol [Internet] 2017 [cited 2023 Mar 4];19(5):699–709. https://doi.org/10.1093/neuonc/now254
Copyright: © 2024 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |