|
|
|
Free Neuropathology 4:7 (2023) |
|
Reflections |
|
Memoirs of a neuropathologist who was unfit to be a clinician |
|
Hitoshi Takahashi |
|
Professor Emeritus (Neuropathology), Niigata University, Japan |
|
Corresponding author: |
|
Additional resources and electronic supplementary material: supplementary material |
|
Submitted: 27 March 2023 |
|
Keywords: Neuropathology, Brain Research Institute Niigata, Reflections, Autobiography |
|
I am very honored to be invited as a contributor to the “Reflections” series for Free Neuropathology. As my English speaking and writing skills are limited, I was initially very hesitant about documenting “my life and my neuropathology career” in English, but I feel it would be a worthwhile task to write about my past without flinching. In undertaking this task, perhaps my main starting point is that I was born into a family completely unrelated to medicine. Origin and Childhood I was born into a farming family in Sendai, Miyagi Prefecture, Japan, in June 1952. The Treaty of San Francisco came into force in April of that year. My father served in Southeast Asia during World War II (WWII). After returning to his family home, he found a national civil service job nearby and took care of his parents. He acknowledged Japan’s responsibility for WWII but did not say much about his wartime experience. My mother, who was also a farmer’s daughter, had experienced the sight of B29 bombers flying over, heading for downtown Sendai when working on their farm. According to my mother, when I was little, I could not stop for a while once I started crying, but did so as soon as I was given a little apple. Since I was a very active and restless baby, my mother left me with my grandmother and went to work on their farm. There was a kindergarten about 600 m from my house on the other side of the railroad crossing. At the age of 5, I went to the kindergarten and got an application for admission by myself, surprising my parents. I remember quite a lot of the year I spent at the kindergarten to which I walked. There were not many cars in those days. I grew up well and healthy. At the age of 7, I enrolled in elementary school. New children were obligated to undergo a chest X-ray examination in accordance with the School Health Act, and this revealed a small shadow on my right lung. An additional gastric juice test for Mycobacterium tuberculosis was negative; this test was not as painful for me as it looked. Eventually, however, I was diagnosed with asymptomatic primary lung tuberculosis and received penicillin injections and oral isonicotinic acid hydrazide (INH) for about one year. A school nurse told me that I should always avoid strenuous exercise. Another piece of advice that stuck me at the time was not to touch the handrails of the stairs unnecessarily. Thereafter, my annual chest X-ray examination revealed no changes in the small lung shadow, and the gastric juice test also remained negative. Finally, the lung lesion was interpreted as an old inflammatory lesion. Throughout my elementary school days, there was no distinction between myself and my classmates in terms of performance in physical education class; I was the fastest runner in my class. My mother had said from the beginning that the small lung lesion was the result of a time I had fallen onto a dirt floor, hitting my chest. In my 5th and 6th grades, I enjoyed playing baseball every Sunday as a member of a local children’ baseball team called the Falcons. One day, a gym teacher asked me whether I knew that Fédération Internationale de Football Association (FIFA) had more members than the United Nations (UN). I underwent two minor surgeries, appendectomy at the age of 9 (Fig. 1) and inguinal hernia repair at the age of 12. Lastly, according to a friend who is a pulmonologist, my mother’s explanation of my lung lesion could not be ruled out, although it no longer matters.
Figure 1: My mother and I in a patient bedroom in a surgical clinic (1961). Education In my junior high school days, I maintained excellent grades. I liked mathematics and English. My father told me that when he was young, he had learned English from a crystal radio set. However, English language education, which attached importance to grammar, was simply a subject to prepare for high school and college/university entrance examinations. Influenced by my gym teacher’s story about FIFA, I began to play football as an extracurricular activity. However, my school’s football team was very weak, and proved unable to score even a single goal in the several games we played. In 1968, I passed the entrance examination for high school (3-year course). The high school that I attended was a public school for boys, and one of the leading preparatory schools in the prefecture. I believe at that time that there were no coeducational high schools in the prefecture. The monthly tuition fee was about 3 US dollars. At my high school, all of the teachers were male – if a few female teachers were present, they escape my memory – and really unique individually. A Japanese teacher told us bluntly during class that he had no responsibility for our willingness to learn, or for our future. I fondly recall the school motto that was expressed by two lines of four “kanji” characters. Although I cannot explain in detail the meaning in English, it made me imagine the way of the scholar rather than that of the samurai. The following year, inspired by the University Student Movements that had started the previous year ago at the University of Tokyo, my high school began a movement for abolition of school uniforms and caps. Many students, including myself, joined the abolition side of the movement. Debates were held between the students and the teachers several times in the gym, and finally we achieved our goal. A mathematics teacher, who was in charge of my class in the 1st and 3rd grades, was on the “conservative” side. I was able to eventually understand his viewpoint; he thought of the students’ parents, who had to worry about what kind of clothes their children should wear. In fact, my mother was a case in point. In the middle of the 3rd grade, my homeroom teacher began worrying about whether I would be able to pass the entrance examination for so-called elite universities. Apparently, I entered the high school with excellent grades. However, even at that point, I was still undecided about my future as the oldest son of a farmer. Or, rather, I began to think about taking a year off from school to study in a preparatory school to enter the university and/or faculty that I wished to attend. In our boys’ high school, there was an attitude that “3 (play well for 3 years) plus 1 (study well for 1 year) equals 4 (a 4-year course high school)”. I liked mathematics, English and world history in particular. However, I have no memory of studying any of those subjects hard during my 3 years. On the other hand, I was a good forward on my school’s football team and enjoyed the games a lot; the football team was really strong and ranked among the top 3 in the prefecture (Fig. 2).
Figure 2: My high school football team (Spring 1970). Front row center: HT with the trophy. Shortly after graduation, my father told me that I had often received care from doctors as a child, and suggested that I might like to become a doctor. I readily seized upon his suggestion without any great thought, but on the condition that I was able to enjoy my university life away from home; I considered that eventually I would have to take care of my parents at home. Therefore, I decided to spend a year preparing for my entrance examinations in a new environment, Tokyo, where my aunt lived. Medical school – Studies and encounters In April 1972, I enrolled at Niigata University School of Medicine. At that time, the tuition fee for one year was about 135 US dollars at all national universities, without any difference between the faculties. The Japanese medical education system was quite different from that of the US, consisting of two courses: 2 years for the medical preparatory course and 4 years for the medical (2-year basic and 2-year clinical) course. In the former, I studied physics, chemistry, biology and other subjects. Although German was a compulsory subject, I was convinced that it would be English from now on in the field of medicine. I finished the 2-year course in 3 years, ending simply in earning enough credits to move on. I joined a football club at medical school, but quit in less than a year because it felt like a small, limited group. I started the 2-year basic course in 1975 and developed a great interest in morphology, including anatomy and pathology. For neuroanatomy, I finished reading a textbook written in English, although it was not thick and had many illustrations. About a year later, I read a book entitled “The Cancer Story” (Iwanami paperback, 1st edn. 1965) written in Japanese by Dr. J. Kamahora, in which I learned about Dr. Fusahiro Ikuta’s research related to the development of cancer (J Neuropathol Exp Neurol 1965; 24: 225-43). Surprisingly, Dr. Ikuta was working at the Brain Research Institute (BRI), Niigata University, where he was professor of pathology. From October to November 1976, there were seven neuropathology classes consisting of lectures and practice (gross and microscopic observation). I still remember the first time that I saw him standing in front of the blackboard in a white lab coat. My neuropathology report, his evaluation sheet with an A-rating and his comment “I wish you good luck” are still treasured. They are the only things remaining from my medical school days. In April 1977, my 2-year clinical course started with practical training. I had been interested in neurosurgery and neurology, but as the days went by I began feeling myself unfit to be a clinician. During my last summer vacation at home as a medical student, my mother told me that I had been originally timid and was perhaps unsuited to be a doctor involved in life and death. I replied to her, “Certainly.” Although most people might take this as a joke, my mother told me seriously, “You should be a dentist.”
Figure 3: Dr. Fusahiro Ikuta in his room (August 13, 1976). He became a professor in 1973. HT took over this room in September 1995. Several months before graduation, I visited Dr. Ikuta at his office in the Department of Pathology, BRI (Fig. 3), and consulted him about my future. I asked him whether I could make a living as a resident of neuropathology. He answered with a smile that I could make a salary as a pathology resident in the University Hospital of the School of Medicine doing locums in local clinics once a week. In addition, he kindly showed me around the Department of Pathology in the BRI. Less than a day later, I decided to become a resident under Dr. Ikuta. My parents had no objection, but asked me what neuropathology was. I graduated from medical school in March 1979, and obtained a medical license at the end of May (all medical license holders are equivalent to MD in Japan). Neuropathology – A choice without hesitation I selected Dr. Ikuta as my teacher and neuropathology as job from which I would make a living. In May 1979, I joined the Department of Pathology at BRI. The BRI is an independent organization/facility within Niigata University. The following month, I became employed as a resident in the Pathology and Laboratory Medicine section of the University Hospital. I was trained in Dr. Ikuta’s lab at the Department of Pathology, where he was a professor and also chair. I also worked in a clinic located in the nearby city every Saturday (a kind of moonlighting) as an assistant to Dr. S. Nakashima (neurologist), my senior in Dr. Ikuta’s lab. Thus, even though the income was low, I became financially independent, and I was happy with that. My residency training was basically on-the-job training in autopsy, brain cutting, biopsy (surgical neuropathology), and histological observation and diagnosis. I came to admire my three seniors, Dr. E. Ohama, Dr. S. Takeda and Dr. Nakashima, as mentors. Case review meetings called neuropathology conferences (NPCs) and brain cutting were held every Thursday morning and afternoon, respectively. Autopsy and biopsy case slides for histological observation were displayed one week in advance. Both residents and graduate students indiscriminately learned diagnosis through autopsy and biopsy cases in the weekly NPCs. Clinicopathological conferences (CPCs) for autopsy cases were also held every month, which was challenging for us as there were many question and answer sessions with neurologists and neurosurgeons. I had a particular interest in the surgical neuropathology of central nervous system (CNS) tumors. It was fun for me, like guessing in a quiz. In fact, my first autopsy patient provided me with a series of precious experiences, including brain cutting, gross observation, microscopic observation, diagnosis, presentation at NPCs and CPCs with discussion, revision, report writing and evaluation. Finally, the autopsy patient, a 9-year-old girl, was diagnosed with a brainstem ganglioglioma. A fortunate event About a year after becoming a resident, Dr. Ikuta told me that I should turn to something new in the form of electron microscope (EM) observation. As if in response to his comment, I had already started EM observation of the brainstem ganglioglioma mentioned above, and several months later I obtained many electron micrographs demonstrating interesting features of the constituent ganglion cells. I have to thank a technician, Mr. S. Egawa, for his guidance on the use of the EM. Early the following year, 1981, I registered an abstract of my ultrastructural study for the 22nd Annual Meeting of the Japanese Society of Neuropathology (JSN) held in Fukuoka in May of that year. Not long after, Dr. Ikuta called me to his room, and suggested I study abroad in New York. Initially, I had serious doubts as to whether I would be up to the task. He told me he had been asked by his old friend, Dr. Kinuko Suzuki, to nominate a young research fellow to help her with EM studies. She was professor of pathology (neuropathology) at Albert Einstein College of Medicine (AECM) in the Bronx, New York. I prepared a simple CV written in English. Before the annual meeting of the JSN, I heard from Dr. Ikuta that I had been officially accepted as a post-doctoral research fellow in Dr. Suzuki’s lab. I was delighted and convinced again that English was the way to go from now on. In August 1981, I left for New York after a send off by many doctors and staff from our Pathology Department at Niigata Station. For some reason, Dr. Ikuta was not able to come; instead of him, Mrs. Ikuta came to see me off. Neuropathology in New York Within a few days of arriving in New York, I rented a two-bedroom apartment located on Davenport Avenue, New Rochelle, near the Atlantic coast under the guidance of Dr. Hitoshi Nagara. I took over the role of Dr. Suzuki’s research fellow from Dr. Nagara, starting my 2-year period abroad. I first visited Dr. Suzuki with Dr. Nagara at the Albert Einstein Rose F. Kennedy Center (Director, Dr. Dominick P. Purpura). There, I found that she and her husband, Dr. Kunihiko (“Kuni”) Suzuki, had adjoining labs on the same floor, and I met 3 (a little later, 3 became 4) Japanese research fellows working under Dr. Kuni. I soon made friends with these Japanese fellows, having conversation entirely in Japanese. I believe that within a few days, Dr. Suzuki introduced me to her colleagues at the Kennedy Center, including Dr. D.S. Horoupian and Dr. C.S. Raine. For a while, people called me “Hitoshi number 2”. Dr. Suzuki showed me “Twitcher” mice, which were used as a murine model of human Krabbe disease (globoid cell leukodystrophy), an autosomal dominant neurological disorder, and roughly explained the future research plan. Looking back on those days, she gave me free access to the EM facility (Fig. 4).
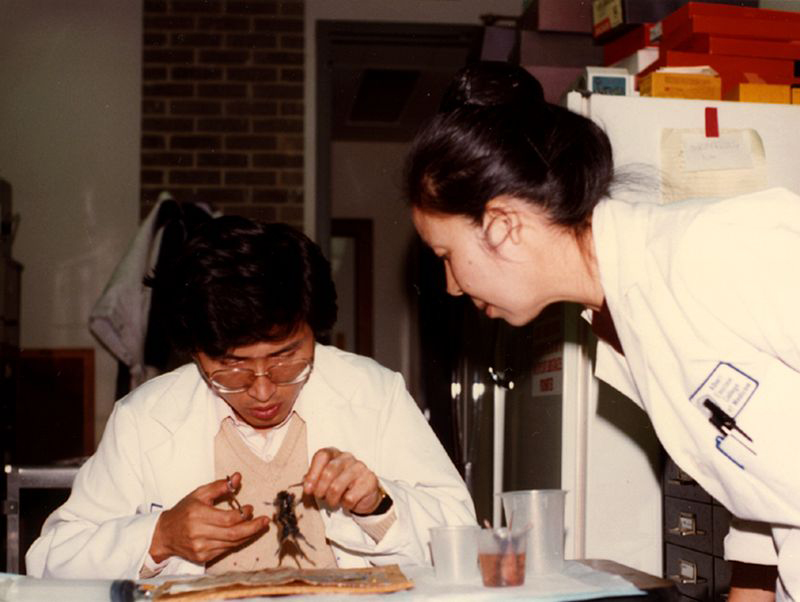
Figure 4: HT dissecting a post-perfusion twitcher mouse with unfamiliar hands and Dr. Kinuko Suzuki keeping her eyes anxiously fixed on the mouse (1981). In 1982, Dr. Suzuki took sabbatical leave in Japan, and I was left in her lab with a technician, Ms. Grace Yuk Gong, for the first half of the year (Fig. 5). During her absence, I spent almost every day except weekends in a dark room. After she returned to the lab, I began preparing my maiden paper in English in parallel with continued EM studies. Armed with an English-Japanese dictionary, I wrote the manuscript on a typewriter. Unlike present-day work using a personal computer, it was a difficult task for me. I truly recognized that there was a big difference between “I like English” and “I use English.” Dr. Suzuki submitted the paper after an intensive review of my repeated manuscript drafts, and it was finally accepted for publication. That night, I toasted alone with a sense of accomplishment in my apartment room.
Figure 5: Neuropathology faculty, residents and fellows at Albert Einstein College of Medicine; note the absence of Dr. K. Suzuki due to sabbatical leave in Japan (May 12, 1982). Front row, left to right: Dr. Shu-Hui Yen, Dr. David Katz, Dr. Robert D. Terry, Dr. Ute Traugott, Dr. Dikran S. Horoupian, Yvonne Kress and Dr. Felicia Gaskin. Top row, left to right: Dr. Peter Davies, HT, Dr. James E. Goldman, Dr. Anne B. Johnson, Dr. David Armstrong, Dr. Cedric S. Rain, Dr. Celia F. Brosnan, Dr. Gary L. Wenk and Dr. Peter Pick. In September of that year, I attended the 9th International Congress of Neuropathology (ICN) held in Vienna, and gave an oral presentation: “An ultrastructural study of oligodendrocytes in the twitcher mouse”. Dr. Ikuta and his colleagues/students also attended the ICN from Niigata, Japan. My senior Dr. Takeda also gave an oral presentation about “Pigmented and non-pigmented neurons in the substantia nigra in Parkinson’s disease (PD)”. One participant raised his hand, gave his name, and asked Dr. Takeda a question. It was at that moment I saw the face of Dr. Kurt A. Jellinger, Editor-in-Chief of Acta Neuropathologica, for the first time. In the symposium on “brain edema”, Dr. Ikuta gave an excellent presentation about the mechanism of lesion repair in brain ischemia using time-lapse images to show the movement of cultured (reactive) astrocytes. I witnessed all of the participants give him a standing ovation at the venue. After the ICN, I joined Dr. Ikuta’s group for a week-long trip around Athens (Fig. 6), Rome, Zurich, Paris and London. Finishing the trip, Dr. Ikuta’s group and I flew back from London Heathrow to Narita and New York John F. Kennedy, respectively. The round trip was a kind vacation gift from Dr. Suzuki, who had also attended the ICN. Back in New York, I began preparing a paper on the topic I presented at the ICN. The paper was accepted for publication through the same process as the previous one.
Figure 6: With the Parthenon, Athens in the background (after the 9th ICN, Vienna, September 12, 1982). Front row, left to right: Dr. Kiyomitsu Oyanagi, Shigekimi Egawa, Dr. Takao Makifuchi, Dr. Yo Oyake and Dr. Kazunori Yamazaki. Top row, left to right: Dr. Yasuji Yoshida, HT, Mrs. Yoshiko Ikuta, Dr. Fusahiro Ikuta, Dr. Shigeru Nakashima, Tomio Ichikawa, Dr. Eisaku Ohama and Dr. Shigeki Takeda. In Dr. Suzuki’s lab at the AECM, I wrote 5 papers as first author under the direction of Dr. Suzuki. I knew nothing about biochemistry/neurochemistry. I was very surprised to see Dr. Hideki Igisu, a research fellow in Dr. Kuni’s lab, grinding the brains of twitcher mice using a homogenizer. However, when I asked him about the morphology of oligodendrocytes, I found that he knew almost nothing about that, either. I was relieved that we shared a similar ignorance of certain areas. From this viewpoint, Dr. Kuni treated me as the second author for a biochemical paper written by Dr. Igisu on the twitcher mouse. This allowed me to study a little about biochemistry/neurochemistry.
Figure 7: Dr. K. Suzuki at HT’s farewell party (April 1983). On returning to Niigata at the end of April 1983, I remembered what Dr. Suzuki had said to me (Fig. 7; also see Fig. 5 in J Neuropathol Exp Neurol 2014; 73: 175-87): “You do not necessarily need scientific papers if you are going to be a good clinician, but you need such papers if you want to be an academician”. I also made many good friends. However, I seldom met non-Japanese foreign friends again, even at subsequent academic meetings. Memories of the Albert Einstein Rose F. Kennedy Center In addition to Dr. Suzuki, two neuropathologists were working at the Albert Einstein Rose F. Kennedy Center for Research in Mental Retardation and Human Development. One was Dr. Horoupian who was in charge of the clinical neuropathology service. The other was Dr. Raine, who was a researcher studying demyelinating diseases, especially multiple sclerosis (MS). Fortunately, I was allowed to participate in the case review meetings held every Monday morning at the Rose F. Kennedy Center led by Dr. Horoupian. On occasion, he would gently ask a resident who was presenting a case, “Why don’t you ··········?” I thought that such a remark beginning with “Why” to each of the residents was one aspect of his cordial educational policies. Dr. J.E. Goldman at the Forchheimer building was a regular member at the weekly meeting. He was a man of few words and always had a rather serious look on his face. I remember that when I passed him in the corridor after my oral presentation at the ICN (Vienna, 1982), he smiled at me and said, “Nice talk.” Dr. R.D. Terry (Department of Pathology, Chair) at the Forchheimer building sometimes also attended the weekly meeting. One day, when a resident was showing a slide of a brain slice from an autopsy case, the diagnosis of which I do not remember exactly, possibly MS, he pointed to the lateral part of the ventricle on the slide and said, “Do you know what here is called in German?” After a moment of silence, I answered, “Wetterwinkel.” He seemed surprised by my answer. I speculated that Dr. Terry’s “Wetterwinkel” came from his teacher, Dr. Harry M. Zimmerman, a pioneer in neuropathology in the US as well as a founder of the AECM, who studied neuropathology under Dr. Walter Spielmeyer in Germany. Dr. Ikuta, Dr. Suzuki and Dr. Terry were all his pupils. While Dr. Suzuki was away, I was especially indebted to Dr. Raine for the use of the EM. I also learned much about oligodendrocytes from him. I already knew that he was very famous in the field of MS. It came as a slight surprise that he was never an arrogant person, but rather a cheerful and somewhat youthful individual, for which I admired him. I saw Dr. Asao Hirano only once or twice at the weekly meetings. However, I had a few opportunities to visit Montefiore Hospital, the University Hospital for the AECM, where I met many Japanese research fellows, including Dr. Imaharu Nakano, Dr. Yoshio Hashizume and Dr. Toshihiko Kubota. Dr. Hirano kindly took me to Dr. Zimmerman’s room and introduced me to him as Dr. Ikuta’s pupil. Of course, Dr. Hirano was also a pupil of Dr. Zimmerman. There are still a large number of Dr. Zimmerman’s second-generation pupils in Japan, including myself. Lastly, Dr. Igisu and his wife often invited me to cheese fondue dinner with wine and to the offer to stay overnight. When I woke up one morning, he told me that I had been talking in English in my sleep. I thought that the reason was either I still liked English or I was already afraid of it. Irrespective, I myself have no memory of “sleep talking”. Based on my experience, I concluded that sleep talking in English is not necessarily the same as speaking English in a dream. Return to Niigata In May 1983, I returned to work as a resident in the University Hospital, and again I worked not in the local clinic, but in the psychiatric hospital every Saturday. Although I was employed as a doctor, I worked as a kind of hospital helper, specifically as an interlocutor for patients, through the courtesy of the director (Dr. Masaharu Tanaka, a former member of our Pathology Department). This gave me the opportunity to see many elderly patients with various forms of dementia such as Alzheimer’s disease (AD). Not long before I started research for a PhD degree, Dr. Nakashima was trying to develop an antibody against tyrosine hydroxylase (TH) for a study of PD using immunohistochemistry (IHC). I became involved in his next project to develop an antibody against serotonin. Finally, using the two antibodies against TH and serotonin and with his help and advice, I began to study the distribution pattern of monoamine neurons in the brainstem of the human fetus using specimens stored at the Brain Disease Research Center (BDRC), the so-called Institutional Brain Bank founded by Dr. Ikuta in 1971. I presented my thesis and obtained a PhD degree from Niigata University in 1985 (Fig. 8). Later, I was very happy to learn that my two papers, one about catecholamine neurons written in Japanese with English abstracts, had been cited in the book The Human Nervous System (George Paxinos, Ed. 1990, Elsevier).
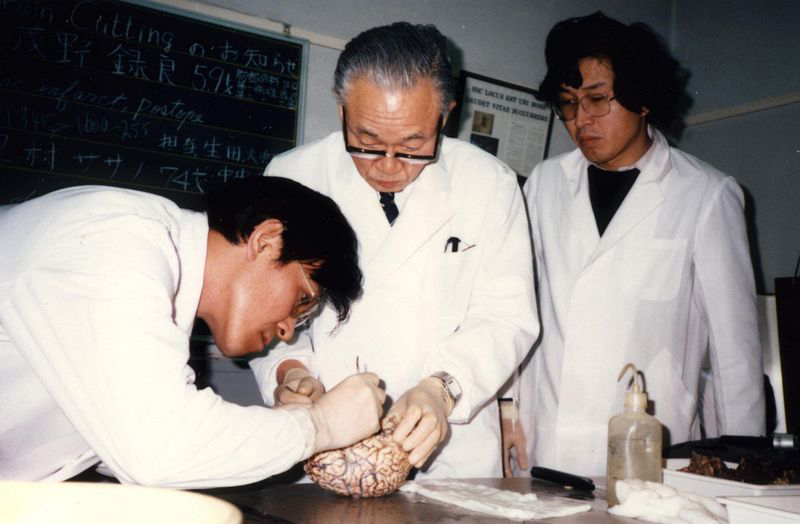
Figure 8: The distribution pattern of serotonin-containing neurons in the midbrain at the level of the caudal portion of the oculomotor nucleus (Brain Dev 1986; 8: 355-65). After a while, I realized that I had one important task remaining: I had promised myself to report the findings I had obtained from my neuropathology autopsy study of young girl in New York. When that paper, entitled “Ultrastructural alterations of neuronal cells in a brain stem ganglioglioma”, was accepted for publication in 1987, I felt that I could finally thank her. Later, I worked on an autopsy case of hereditary dentatorubral-pallidoluysian atrophy (DRPLA), a clinicopathological entity that had been established by Dr. Haruhiko Naito and Dr. Shinsaku Oyanagi at Niigata University. This autopsy case was the second one in the same family with DRPLA, and the report on the two autopsy cases from different generations provided an opportunity to promote later collaboration between the Departments of Neurology and Neuropathology at BRI. I had also developed a great interest in progressive supranuclear palsy (PSP) through the EM work, which had revealed 15-nm-wide straight tubules in various regions of the brain. Another aspect of great importance was learning to carry out quantitative analysis of neurodegenerative diseases from my senior Dr. K. Oyanagi, who kindly involved me as a collaborator for his research on AD, PSP, and other diseases. I knew that Dr. Terry had emphasized the importance of quantitative morphometric analysis, including cell counts, in a study of senile dementia of the Alzheimer type (Annual Meeting of American Association of Neuropathologists (AANP), Philadelphia 1982), but I had not been interested in such methodology at that time. My experiences up to that point had only involved autopsy and biopsy, in a sense the patients concerned were largely faceless, and merely provided me with an opportunity to write papers. Therefore, I was convinced that I was unfit to be a clinician who had to work with living patients suffering from illness. Moreover, I became interested in neurodegenerative diseases such as PD, PSP and AD, in addition to surgical neuropathology as routine work (Fig. 9). My experiences at the psychiatric hospital may have contributed to the change in my academic interest.
Figure 9: Brain cutting at the Brain Research Institute (December 19, 1985). From left: Dr. E. Ohama, Dr. F. Ikuta and HT. With my junior fellows After returning to Niigata, I came to have junior fellows working around me. They were mostly graduate students studying for their PhD under Dr. Ikuta, and came to see me as an “elder brother” in our Pathology Department. I had various discussions with them about our future, specifically about the need to report our achievements in English if possible, regardless of whether it involved case studies or original work. They were excellent individuals, and all imbued with the spirit of “learn well and play well”. At night after work, we sometimes talked together about our research while drinking at the pub. The pub owner often said to us, “What’s so funny about ‘talking shop’ while drinking?” My junior fellows were Kazuhiko Watabe, Shinji Ohara, Mitsunori Yamada (Fig. 10), Kensuke Kawai, Koichi Wakabayashi (Fig. 11) and Akiko Furuta. I have two memorable episodes from my second residency when I was focused on neuropathology. I came to be involved indirectly in a study by my junior, Dr. Ohara, who was a neurologist with an interest in peripheral nerves, studying ultrastructural changes in perineurial cells in Wallerian degeneration using mouse phrenic nerves. He often showed me electron micrographs and asked me to comment on the findings. He submitted a paper to a well-known pathology journal at my suggestion. One of the two reviewers requested an additional experiment for acceptance. I advised him that there was no need for such an experiment. When he received a letter of acceptance from the Editor-in-Chief, I was very relieved; the paper was accepted without difficulty in September 1985. It became my first collaborative study with a junior fellow.
Figure 10: Good fellows (April 26, 1984). From left: Dr. Mitsunori Yamada, Dr. Shinji Ohara and HT.
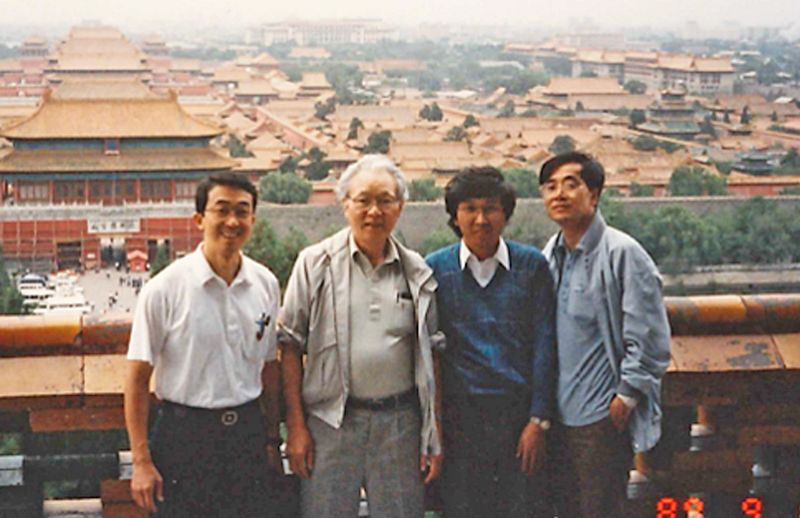
Figure 11: Dr. Lysia K.S. Forno and Dr. Koichi Wakabayashi at the 13th ICN in Perth (September 8, 1997). All of us working in Dr. Ikuta’s lab experienced a very big event. Dr. Wakabayashi found Lewy bodies (LBs) outside the brain in Auerbach’s and Meissner’s plexuses in the alimentary tracts of autopsied patients with PD – a discovery that overturned the conventional concept of the disease. I admired his observational skills, and this experience reaffirmed the maxim that seeing is believing. I spent a lot of valuable time with him in the paper-writing process. The paper was submitted at the end of 1987 and accepted after minor revision in February of 1988. I was very honored to be included as a co-author. Faculty position in neuropathology By 1987, it had been 9 years since I started my life as a resident in the University Hospital. At that time, I started to think about my future seriously from time to time, and always came to the conclusion that I should become a pathologist instead of a neuropathologist. Even now, the former is in much higher demand nationwide. However, my feeling that I was unfit to be a clinician remained unchanged. Then, in May 1988, there was a sudden change in our Pathology Department, and I obtained a full-time faculty position, assistant professor. Later, in October 1991, I was promoted to associate professor under similar circumstances. In late May 1988, shortly after I had become an assistant professor, Dr. Ikuta arranged for Dr. Jellinger and Dr. Georg W. Kreutzberg to visit our Pathology Department (see Fig 7 in: Free Neuropathol 2020; 1: 25). At that time, I was preparing to submit a paper on “Neuroendocrine markers in central nervous system neuronal tumors” with an office worker. As if peeking from behind, Dr. Jellinger said to me, “Why not send it to Acta?” In the evening, he delivered a lecture on “Neuropathology of Rett syndrome.” I asked him a question about the substantia nigra lesion, but unfortunately I do not remember the details of either my question or his answer. The above paper was accepted for publication in Acta Neuropathologica on July 28, 1988. Regardless of my faculty position, I continued my studies freely. In fact, it was always of great interest for me to observe autopsy and biopsy cases. At some point, I encountered an autopsy case that determined a future research subject. My diagnosis for that case was “atypical motor neuron disease” (MND): it did not matter to me whether the disease was called MND or amyotrophic lateral sclerosis (ALS). The point was that neuron loss was also evident in the non-motor neuron systems. In addition, Bunina bodies (BBs) were detected not only in the lower motor neurons but also in subthalamic neurons. Thereafter, I also had an opportunity to report the clinicopathological features of two familial neurological disorders. One was familial ALS with SOD1 mutation; it is a good example of the rebirth of an old case that had slept for a long time in the BDRC under the diagnosis of familial ALS with posterior column involvement. The other case was autosomal-recessive juvenile parkinsonism in a family, with neuropathological findings for one individual; the familial disease was later found to be linked to PARK2 (Parkin). It was my pleasure to receive requests for joint research from both inside and outside the BRI. In this context, I would like to mention three intra-institutional collaborative studies in my early professional career. The first was a clinicopathological study on “Cerebral glioblastoma with cerebrospinal fluid dissemination” proposed by Dr. Kiyoshi Onda in the Department of Neurosurgery. The paper was published in 1989 with favorable comments from Dr. Lucien J. Rubinstein. Dr. Rubinstein, together with Dr. Scott R. Vandenberg, visited to our Pathology Department in May 1984. The second was an experimental study of “Remote astrocytic response of the prefrontal cortex to lesions in the nucleus basalis of Meynert" using rats. It was designed by Dr. Katsuhiko Yanagisawa in the Department of Neurology, and was of great interest to me when considering the pathological picture of cholinergic deafferentation in AD. The last was a genetic study, “Causative gene analysis of hereditary DRPLA”, led by Dr. Shoji Tsuji in the Department of Neurology, in which unstable expansion of a CAG repeat in chromosome 12 was identified as being responsible for the familial disease. Like the case of familial ALS with SOD1 mutation, the aspect of greatest significance for me was that frozen brain tissues from autopsy-proven patients stored in the BDRC were also used in the genetic analysis. Working with a Chinese friend In our Pathology Department, there was a Chinese neurologist named Mu-Yi Wang from China Medical University in Shenyang, who joined us in October 1980 and studied neuropathology under Dr. Ikuta. He was a government-sponsored international student from China in the era of reform and opening up. We soon became good friends, and often talked about not only neuropathology but also Chinese history. He was a sincere and kind gentleman who always had a smile on his face. In late 1981, I received an airmail letter with attached massages from all the lab members, in which Dr. Ikuta said “Make a lot of good friends” and Dr. Wang said “We will meet again”. Dr. Wang left for China in March 1982 when I was still in New York. An opportunity came for me to meet Dr. Wang again when Dr. Ikuta received a Grant-in-Aid for his scientific research entitled “Joint Study on Demyelinating Disorders between Japan and China” from the Ministry of Education, Science and Culture (Monbusho). Dr. Ikuta, Dr. Oyanagi and I met Dr. Wang again at Beijing airport in September 1989, the year of the Tiananmen Square Incident. He greeted us with a warm smile, saying “Nice to see you again,” in Japanese. During the trip, he helped us as an interpreter of Chinese (Fig. 12).
Figure 12: With the Forbidden City in the background (September 15, 1989). From Left: Dr. K. Oyanagi, Dr. F. Ikuta, HT and Dr. Mu-Yi Wang at Jingshan Park in Beijing. Dr. Oyanagi and I accompanied Dr. Ikuta on research trips in September 1989 and October 1991. We visited the medical schools in Shanghai, Chongqing, Changchun and Shenyang in 1989, and those in Suzhou, Nanjing, Hefei, Wuhan, Xian, Beijing and Harbin in 1991. The cases selected and presented by the Chinese side allowed us to observe many typical examples of Baló’s disease. When visiting Norman Bethune University of Medical Science in Changchun in 1989, I met two young men, Dr. Mu Su and Dr. Da-Lin Yao, both of whom wanted to study aboard. Dr. Su joined our Pathology Department in BRI as a Monbusho scholarship student in May 1992 and finally obtained a PhD degree from Niigata University in 1997. Since then, he has worked as a pathologist in the US for many years. The name Da-Lin Yao appeared as the first author in a paper on “Concentric sclerosis (Baló)” published in 1994. I still believe that it was him I met in Changchun. He must have studied neuropathology under Dr. H.D. Webster at National Institutes of Health (NIH). In 1991, we met Dr. Ke-Wei Huang and Dr. Lu-Ning Wang at the Chinese People’s Liberation Army General Hospital. It was said that Dr. Huang was a pioneer of Neuropathology in China and that Dr. Wang was his favorite disciple. In deep sorrow About a year after I was promoted to associate professor, a tragedy fell upon me. When I came home from my off-campus work in the evening and opened the front door of my house, the phone rang. When I picked up the phone, my junior colleague, Dr. Yamada, informed me that my wife Shizue had been hit by a car on the way home and taken to the hospital by ambulance. She developed a subdural hematoma and underwent emergency surgery. Thereafter, almost every day, I spent my lunch breaks and about an hour after 5:00 p.m. by her bedside talking to her, but she never regained consciousness. People around me used to say that they could not be like me. I always replied that it was easier for me to act the way I did. My love for her was why I was able to devote the rest of my time to neuropathology. Years later, I recall trying to look her in the eyes and blink my own eyes three times. It was not so long before she began responding to me by blinking her own eyes three times. As a neuropathologist, I still do not fully understand her behavior or reaction; rather, I have not yet found a satisfactory answer as to whether or not she regained any degree of consciousness. At the end of February 1999, about 7 years after the car accident, she passed away surrounded by myself and relatives. In the meantime, Dr. Ikuta retired from his faculty position at Niigata University at the age of 65 in late March 1995 and became professor emeritus the following April. Almost half a year later, in September 1995, I was elected as his successor and became Professor in the Department of Pathology, BRI, Niigata University. I told my wife and parents about this. Shizue seemed to smile a little. To my mother, it would not have meant much: rather, she might have been saddened by my decision to settle in Niigata. So ultimately, I did not fulfill my parents’ expectation of caring for them at home, and my younger brother took over that role. Professorship In Japanese medical schools, one department generally has one professor, one associate professor and two assistant professors. The professor also serves as a chair to take responsibility for departmental management. This meant that I was no longer simply a neuropathologist/researcher in the Department of Pathology. At first, I confirmed that our neuropathology was based on autopsy and biopsy as a routine form of work, just as it had been before. Needless to say, as far as possible, there was no limit to individual study subjects/topics and methods. This meant that there was no change in the daily work of the faculty. On the other hand, the responsibility of teaching residents and graduate students, and supporting their research, weighed heavily on my shoulders. To meet this responsibility, I had to do my best to obtain funds and keep them flowing. Fortunately, in this respect, I remained successful until my retirement. Overall, I was blessed with excellent human resources, including the faculty and staff as well as the residents and graduate students, in the wonderful setting of the BRI inherited from our predecessors, including Dr. Ikuta, for which I was extremely grateful. Chinese students and academic exchange with China Shortly after I became professor, I communicated with Dr. Wang in Shenyang, China, by phone. In return for his friendship, I wanted his pupil to study neuropathology as a graduate student in our Pathology Department. This resulted in his favorite disciple, Dr. Yue-Shan Piao, coming to Niigata in September 1997 after completing a master course at the China Medical School in Shenyang, and then enrolling in a PhD course in April 1998. My teaching career started with her. She had a strongly inquisitive mind and a competitive personality. Thereafter, I accepted a number of Chinese graduates in medicine as graduate students for a PhD course or as short-term international students. All of these students studied neuropathology well and enjoyed living in Japan. In May 2003, through Dr. Piao’s mediation, I was invited to China for the first time to celebrate the 25th Anniversary of the Founding of the Neurological Clinicopathological Conference in Beijing. This was the beginning of my academic exchange with China, and allowed me to became reunited with Dr. L-N Wang for the first time in 12 years. She had since become a leader in neurology and related neuropathology in China. She told me that it was very difficult to have an opportunity to obtain autopsy cases in China. I immediately surmised that this was related to Confucianism. Dr. Piao returned to China in July 2004 and began a new path as a neuropathologist under Dr. De-Hong Lu in the Department of Pathology, Xuanwu Hospital, Capital Medical University. Thereafter, I was often invited to conferences related to neuropathology in China. In 2005, I was invited to China twice: Beijing (Fig. 13) and Changsha in April, and Beijing and Shanghai in September. I have a fond memory of presenting a lecture on “The importance and fascination of neuropathology” to young participants at a Chinese Neuropathology Education Seminar held in Beijing in September 2005. I could feel great vitality in the young listeners.
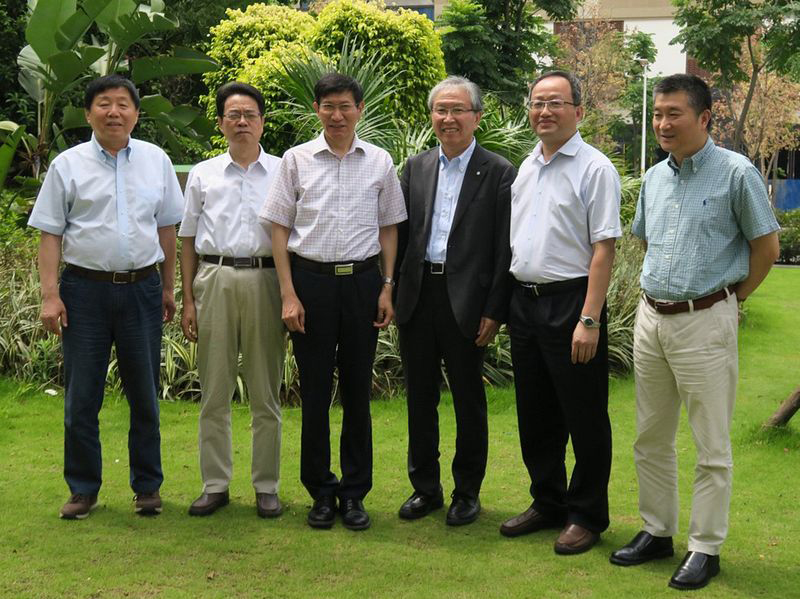
Figure 13: At Xuanwu Hospital, Capital Medical University in Beijing (April 5, 2005). From left: Dr. De-Hong Lu, HT and Dr. Lu-Ning Wang. Since 2008, I attended the Annual Chinese Neuropathology Case Conference, giving me an opportunity to make new friends in the Chinese neuropathology group. So far, I have observed many interesting CNS tumors directly by light microscopy. At the venue, young participants, including residents and graduate students, listened intently to each presentation and during the following discussion, and some of them took pictures of the projected images on smart phones. The leaders placed strong importance on discussion of the findings and diagnoses (Fig. 14). At the dinner party, both young and old participants were very frank and friendly. When talking, they did not appear to care about each other’s age or status; the atmosphere was similar to what I had experienced in New York.
Figure 14: With leaders of the Chinese neuropathology group in Fuzhou (June 13, 2018). Left to right: Dr. D-H Lu (Beijing), Dr. Shi-Zhu Yu (Tianjin), Dr. Xiu-Wu Bian (Chongqing), HT, Dr. Sheng Zhang (Fuzhou) and Dr. Yin Wang (Shanghai). Although not shown here, this group also has several female leaders. Unfortunately for me, presentations of autopsy cases, including those of neurodegenerative diseases, were extremely rare at the conference. Almost certainly, the leaders’ specialty was surgical neuropathology dealing with CNS tumors and allied diseases. Since 2015, Dr. Piao has been Professor in the Department of Pathology, Capital Medical University in Beijing, and she must be now one of the leading researchers of neuropathology in China. Unfortunately, since 2020, the annual conference on site has been canceled due to the COVID-19 pandemic. Neurodegenerative diseases My study of neurodegenerative diseases began with an autopsy case that made me take a closer look. My passive attitude was the exact same as that of a clinician was waiting for a patient in the examination room. In fact, my high school classmates had often told me that if I were a clinician, I would have made a good practitioner. Therefore, autopsy studies often ended with a single case report, although I still believe that such studies are very important for the teaching of residents and graduate students. Occasionally, however, a single case report developed into a study subject or topic as similar autopsy cases accumulated in the BDRC. Although I forget the specific situation, I saw Gallyas-positive argyrophilic glial cells in the midbrain of a PD patient using light microscopy. I immediately confirmed the finding with Dr. Wakabayashi. My interest in PD then skyrocketed. In the following year, 1997, an α-synuclein mutation was identified as being responsible for familial PD with LBs. Shortly afterwards, I had the opportunity to discuss the discovery with Dr. Makoto Yoshimoto, with whom a joint research project was undertaken. I was very surprised to hear that he had anti-NACP (human α-synuclein) antibodies that he had developed him-self. Another joint study was soon initiated, and this was reported as “NACP, a presynaptic protein, immunoreactivity in LBs in PD” in 1997. Although our report fell a little behind another group, our interest in α-synuclein (NACP) did not end there. By the end of the year, our target had shifted to multiple system atrophy (MSA). Dr. Wakabayashi’s contribution to PD and MSA research was significant. Since February 2000, he has been professor in the Department of Neuropathology, Institute of Brain Science, Hirosaki University School of Medicine, Hirosaki. It is worth mentioning that Dr. K. Iwanaga was the first to report the occurrence of α-synuclein-positive aggregates in the cardiac plexus of both patients with PD and those with incidental LB disease. The study of hereditary DRPLA in collaboration with Dr. Tsuji’s group also progressed smoothly; it started with IHC using anti-ubiquitin antibody and later developed to the use of monoclonal anti-polyglutamine antibody (1C2). Finally, Dr. Hayashi (later Toyoshima) and Dr. Yamada made significant contributions in the wider area of polyglutamine diseases beyond hereditary DRPLA. They never forgot the necessity of EM observation in parallel with IHC. Since April 2015, Dr. Yamada has been professor in the Department of Brain Disease Research, Shinshu University School of Medicine, Matsumoto. I also carried out a study of DRPLA with the help of my colleagues, as the topic “Neuronal nuclear alterations in DRPLA” seemed plain and uninteresting to them. However, a photograph used in the report graced the cover of Brain Research, where it was accepted for publication. I felt like I had received a medal and was very happy; a feeling shared by the other staff of our Pathology Department. Another study was on four-repeat (4R) tauopathies, involving many colleagues, including graduate students. When I first had an autopsy case diagnosed clinically as PSP, it was a fairly rare neurological disorder in Japan. I remember that at the invitation of a neurologist, I observed a wheelchair-bound male patient with PSP, and could see at a glance there was marked nuchal dystonia. At that time, I had been unfamiliar with the neurological term dystonia. At present, PSP is known to demonstrate a wide pathological and clinical spectrum as a representative 4R tauopathy. To my surprise and great pleasure, Dr. Hayashi (Fig. 15) found a novel tau gene mutation (exon1, Arg5His) responsible for late-onset frontotemporal dementia. He had taught me how to operate a personal computer, and I believed that he had a flair for genetic research. Globular glial tauopathy (GGT) is a new category within the 4R tauopathies; we were able to collaborate to establish and strengthen the disease concept; Dr. Piao, Dr. Fu, Dr. Tanaka and Dr. Toyoshima played an important role in this.
Figure 15: With the Po River in the background at the 15th ICN in Turin (September 13, 2003). Front row, left to right: HT, Dr. Shintaro Hayashi and Dr. Akiyoshi Kakita. Top row, left to right: Mrs. Yuriko Takahashi, Dr. Chun-Feng Tan, Dr. Chikanori Inenaga and Dr. Koichi Kawasaki. CNS tumors As mentioned already, the diagnosis of CNS tumors was intriguing and sometimes challenging for me. Among works of my generation, there were several authorities on the diagnosis of CNS tumors, including Dr. Rubinstein. I remember Dr. Rubinstein giving an oral presentation on “Astroblastoma” with slides of elegant electron micrographs. Surprisingly, he performed the presentation by reading the manuscript prepared. I felt that he was a noble gentleman rather than a well-known authority (Annual meeting of the AANP, Dallas 1989). I also admired Dr. Jacques Hassoun and Dr. Bernd W. Scheithauer for their sharp diagnostic eye for CNS tumors. My sense of enthusiasm was often shared with my residents and graduate students as case reports, in which we also showed the ultrastructural features of individual cases. Our case reports included those on a range of notable CNS tumors, including ganglioglioma, pleomorphic xanthoastrocytoma, tanycytic ependymomas, melanotic cerebral astrocytoma, atypical teratoid/rhabdoid tumor, chordoid glioma of the third ventricle, and astroblastoma. For diagnosis of CNS tumors by biopsy, I got into the habit of looking at the specimen first. For example, in glioblastomas in the thalamus, the patient’s age could often be inferred and confirmed later by the clinical history. This was also the case for brainstem (pontine) gliomas, although biopsy was very unusual in such cases. I was curious as to which gene determined the location (thalamus) as well as the age of onset (children/adolescent). The gene associated with such gliomas has already been discovered. Research on CNS tumors awaits the next development, although the same can be said for neurodegenerative diseases. Minamata disease and brain development Niigata is famous as the “Snow country” described by Yasunari Kawabata (Nobel Laureate, 1968) in his novel. Unfortunately, the name is also associated with Minamata disease, a neurological disease caused by methylmercury poisoning. I was involved in “Research on the effect of mercury on the nervous system, etc. (1996-2009)” commissioned by the Ministry of the Environment. Our study group led by Dr. Kakita (Fig. 15) conducted experiments designed to clarify the pathomechanism of Minamata disease using rats treated with methylmercury, focusing especially on intrauterine and fetal brain development. Joint studies with Dr. Mineshi Sakamito at the National Institute for Minamata Disease (NIMD) (Director, Dr. Komyo Eto), Minamata, also yielded new biochemical and behavioral data through similar experiments. I visited Minamata several times for meetings with the faculty at NIMD. Although I already had knowledge of the disease, I was able to witness for myself the scale of the pollution damage on the population, which far exceeded that in Niigata in terms of both number and degree. When I visited with Chinese graduate students, I showed them the birthplace of Minamata disease and the Minamata Disease Municipal Museum. I am sure that at the time, various pollution-related problems in China, including Minamata disease, were receiving international attention. I have visited the Nursing Home for patients with childhood Minamata disease, and I will never forget their haunting gaze; they were about the same age as myself. Dr. Kakita also developed research on the neuropathology of epilepsy, which is often associated with focal cortical dysplasia, in our Pathology Department. He supported me in every aspect of my professional career as a professor. Since April 2018, Dr. Kakita has been my successor as professor in the Department of Pathology, BRI, his alma mater. At present, he serves as President of the JSN. Amyotrophic lateral sclerosis – Final lecture by a retiring professor I think that there is a custom of German origin whereby a retiring professor in Japan delivers a final lecture. It has been said that retiring professors tend to give lectures on the outputs of their research resulting from passion and hard work. The title of my final lecture was “Amyotrophic lateral sclerosis (ALS): before and after the discovery of TDP-43.” It was not a story of hardship, however. In ALS, there are two characteristic neuronal cytoplasmic inclusions: BBs and skein-like and/or round spherical inclusions. The latter are clearly shown to be ubiquitin-positive inclusions (UPIs) by IHC. Interestingly, UPIs are sometimes also demonstrable in the temporal lobe, being significantly associated with dementia. I experienced a crossroads in promoting joint research on ALS. Considering the number of neurons bearing UPIs, I always maintained that UPIs in the temporal lobes, and not those in the anterior horns, were targets for identification of the pathological protein involved in ALS. However, a molecular biologist partner wanted to select BBs in the anterior horn cells. At that time, a technique for capturing and analyzing single cells from the brain sections had already been established. The large anterior horn cells bearing BBs were easy for my partner to focus on, as he had both the equipment and the technology for the task. I could understand his research spirit, because I was still keen to understand the nature and origin of BBs. However, the discussion of joint research came to end. In September 2006, I attended the 16th ICN in San Francisco. Leaving the room with a smile after listening to a lecture on PD by Dr. J. William Langston, I was tapped on the shoulder from behind. When I turned around, I was told by my friend, Dr. Paul G. Ince, that the protein component of the UPIs in ALS had been finally identified, and that the report was in press. On the plane on the way back to Japan, I thought that a series of related studies might already be underway. Soon afterwards, I read the paper on the discovery of the pathological protein, TDP-43. However, after waiting for a few months, no follow-up papers appeared. Eventually, I called a graduate student, Dr. Tan (Fig. 15), to my room and told her that although it might be too late to do this study, we should start it. As a result, we were the first to show the distribution pattern of TDP-43-positive neuronal cells, together with occasional glial cell involvement, in sporadic ALS. I do not have any particular objection to the theory/hypothesis – “conformational disease” and “prion-like pathomechanism” – of neurodegenerative diseases such as AD (amyloidopathy/tauopathy), PD (α-synucleinopathy) and ALS (TDP-43 proteinopathy). However, I consider that ALS is quite different from the other two diseases, AD and PD, concerning the pattern of the pathological protein propagation. At the end part of the lecture, I also mentioned GGT, which is a sporadic 4R tauopathy showing a feature of MND/ALS, i.e. upper and lower motor neuron involvement. In our research on ALS and 4R tauopathies, Dr. Osamu Onodera (Department of Neurology) and Dr. Takeshi Ikeuchi (Department of Molecular Genetics) were often important collaborators at the BRI. Our published papers covered in my final lecture were as follows.
1. Takahashi H, Ohama E, Ikuta F, Tokiguchi S. An autopsy case of atypical motor neuron disease with Bunina bodies in the lower motor and subthalamic neurons. Acta Pathol Jpn 1991; 41: 46-51. 2. Takahashi H, Oyanagi K, Ohama E, Ikuta F. Clarke's column in sporadic amyotrophic lateral sclerosis. Acta Neuropathol 1992; 84: 465-70. 3. Takahashi H, Oyanagi K, Ikuta F. The intermediolateral nucleus in sporadic amyotrophic lateral sclerosis. Acta Neuropathol 1993; 86: 190-2. 4. Takahashi H, Makifuchi T, Nakano R, Sato S, Inuzuka T, Sakimura K, Mishina M, Honma Y, Tsuji S, Ikuta F. Familial amyotrophic lateral sclerosis with a mutation in the Cu/Zn superoxide dismutase gene. Acta Neuropathol 1994; 88: 185-8. 5. Piao YS, Wakabayashi K, Kakita A, Yamada M, Hayashi S, Morita T, Ikuta F, Oyanagi K, Takahashi H. Neuropathology with clinical correlations of sporadic amyotrophic lateral sclerosis: 102 autopsy cases examined between 1962 and 2000. Brain Pathol 2003, 12: 10-22. 6. Toyoshima Y, Piao YS, Tan C-F, Morita M, Tanaka M, Oyanagi K, Okamoto K, Takahashi H. Pathological involvement of the motor neuron system and hippocampal formation in motor neuron disease-inclusion dementia. Acta Neuropathol 2003; 106: 50-6. 7. Tan CF, Eguchi H, Tagawa A, Onodera O, Iwasaki T, Tsujino A, Nishizawa M, Kakita A, Takahashi H. TDP-43 immunoreactivity in neuronal inclusions in familial amyotrophic lateral sclerosis with or without SOD1 gene mutation. Acta Neuropathol 2007; 113: 535-42. 8. Nshihira Y, Tan CF, Onodera O, Toyoshima Y, Yamada M, Morita T, Nishizawa M, Kakita A, Takahashi H. Sporadic amyotrophic lateral sclerosis: two pathological patterns shown by analysis of distribution of TDP-43-immunreactive neuronal and glial cytoplasmic inclusions. Acta Neuropathol 2008, 116: 169-82. 9. Nishihira Y, Tan CF, Hoshi Y, Iwanaga K, Yamada M, Kawachi I, Tsujihata M, Hozumi I, Morita T, Onodera O, Nishizawa M, Kakita A, Takahashi H. Sporadic amyotrophic lateral sclerosis of long duration is associated with relatively mild TDP-43 pathology. Acta Neuropathol 2009; 117: 45-53. 10. Takeuchi R, Tada M, Shiga A, Toyoshima Y, Konno T, Sato T, Nozaki H, Kato T, Horie M, Shimizu H, Takebayashi H, Onodera O, Nishizawa M, Kakita A, Takahashi H. Heterogeneity of cerebral TDP-43 pathology in sporadic amyotrophic lateral sclerosis: evidence for clinic-pathologic subtypes. Acta Neuropathol Commun 2016; 4: 61. 11. Kimura T, Jiang H, Konno T, Seto M, Iwanaga K, Tsujihata M, Satoh A, Onodera O, Kakita A, Takahashi H. Bunina bodies in motor and non-motor neurons revisited: a pathological study of an ALS patient after long-term survival on a respirator. Neuropathology 2014; 34: 392-7. 12. Yokoseki A, Shiga A, Tan CF, Tagawa A, Kaneko H, Koyama A, Eguchi H, Tsujino A, Ikeuchi T, Kakita A, Okamoto K, Nishizawa M, Takahashi H, Onodera O. TDP-43 mutation in familial amyotrophic lateral sclerosis. Ann Neurol 2008; 63: 538-42. 13. Konno T, Shiga A, Tsujino A, Sugai A, Kato T, Kanai K, Yokoseki A, Eguchi H, Kuwabara S, Nishizawa M, Takahashi H, Onodera O. Japanese amyotrophic lateral sclerosis patients with GGGGCC hexanucleotide repeat expansion in C9ORF72. J Neurol Neurosurg Psychiatry 2013; 84: 398-401. 14. Kosaka T, Fu YJ, Shiga A, Ishidaira H, Tan CF, Tani T, Koike R, Onodera O, Nishizawa M, Kakita A, Takahashi H. Primary lateral sclerosis: upper-motor-predominant amyotrophic lateral sclerosis with frontotemporal lobar degeneration - immunohistochemical and biochemical analyses of TDP-43. Neuropathology 2012; 32: 373-84. 15. Fu YJ, Nishihira Y, Kuroda S, Toyoshima Y, Ishihara T, Shinozaki M, Miyashita A, Piao YS, Tan CF, Tani T, Koike R, Iwanaga K, Tsujihata M, Onodera O, Kuwano R, Nishizawa M, Kakita A, Ikeuchi T, Takahashi H. Sporadic four-repeat tauopathy with frontotemporal lobar degeneration, Parkinsonism, and motor neuron disease: a distinct clinicopathological and biochemical disease entity. Acta Neuropathol 2010; 120: 21-32 16. Tanaka H, Toyoshima Y, Kawakatsu S, Kobayashi R, Yokota O, Terada S, Kuroda S, Miura T, Higuchi Y, Otsu H, Sanpei K, Otani K, Ikeuchi T, Onodera O, Kakita A, Takahashi H. Morphological characterization of glial and neuronal tau pathology in globular glial tauopathy (Types II and III). Neuropathol Appl Neurobiol 2020; 46: 344-58. 17. Takeuchi R, Toyoshima Y, Tada M, Tanaka H, Shimizu H, Shiga A, Miura T, Aoki K, Aikawa A, Ishizawa S, Ikeuchi T, Nishizawa M, Kakita A, Takahashi H. Globular glial mixed four repeat tau and TDP-43 proteinopathy with motor neuron disease and frontotemporal dementia. Brain Pathol 2016; 26: 82-94. Leadership – domestic and international Our BRI is the only research institute at Niigata University, established in 1967, for the study of theories concerning the brain and brain diseases (Fig. 16). I served as Director of the BRI for about 12 years (2002-2014). A year before I became Director, the 21st Century Center of Excellence (COE) Program was initiated as a project of the Ministry of Education, Culture, Sports, Science and Technology (MEXT). In a BRI faculty meeting, I was asked to act as a leader of the project, supported by the University President. In response, I decided to apply for the COE Project with the help of Dr. Tsutomu Nakada, Head of the Center for Integrated Human Brain Science, BRI. The aim of the project, entitled “Center for Brain Pathology Research and Education (2002-2008)” was to form a world-class base for research and education in the field of neuropathology. In 2007, we held the Neuropathology International Symposium at the BRI, and this was one of the great achievements of the MEXT-supported COE project. To learn about current research and practice in neuropathology, we invited 15 foreign experts to the symposium, who delivered lectures on their specialist topics (Fig. 17).
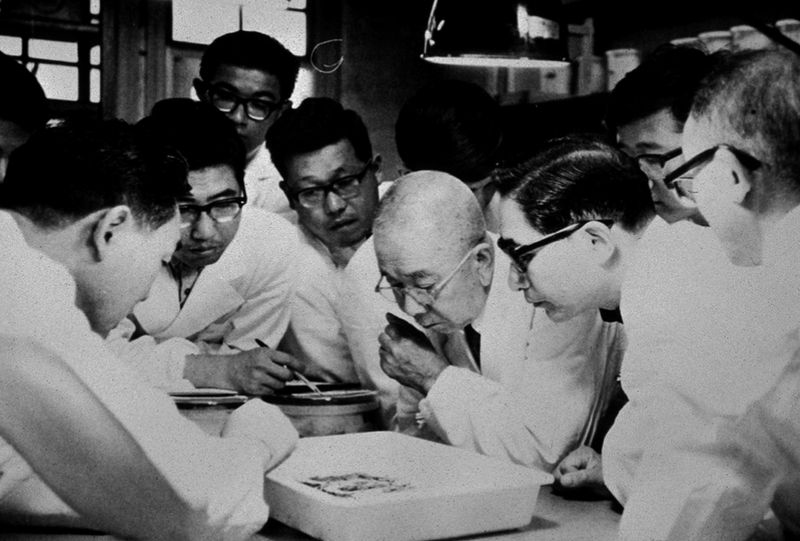
Figure 16: Brain cutting at the Brain Research Institute (June 21, 1971). Front left: Dr. F. Ikuta (42 years old). Front row, right to left: Dr. Tatsuji Ito (pathologist, 67 years old), Dr. Komei Ueki (neurosurgeon, 57 years old) and Dr. Mizuho Nakata (neurosurgeon, 78 years old). These three are Dr. Ikuta’s teachers.
Figure 17: Neuropathology International Symposium in Niigata (October 27, 2007). 2nd row, left to right: Drs. Bernd W. Scheithauer (USA), Takanori Hirose, Gregory N. Fuller (USA), Markus Glatzel (Germany) and Herbert Budka (Austria). 3rd row, left to right: Drs. Wieslawa Grajkowska (Poland), A. Kakita, skipping one person and Thong K. Wong (Malaysia), Francoise Gray (France) and Tumtip Sangruchi (Thailand). 4th row, left to right: Drs. M. Yamada, K. Wakabayashi, Paul G. Ince (UK), Dennis W. Dickson (USA), James C. Vickers (Australia), Min-Cheol Lee (Korea), Chitra Sarkar (India) and Chin-Chen M. Lee (Taiwan). 5th row, 2nd left to right, Drs. D-H Lu (China), Yasuo Sugita, Yoshio Hashizume, Toru Iwaki, skipping one person and HT, F. Ikuta and E. Ohama. 6th row, 4th from left, Dr. Yoichi Nakazato and 1st from right, Dr. Shinya Tanaka. Except Dr. F. Ikuta, only speakers and chairs are named. The JSN was established in 1960 through the efforts of neurologists, psychiatrists and neuropsychiatrists working at various medical schools. I served as President of the JSN for a relatively long period (2010-2018). My greatest concern was that there were only a small number of departments and faculties related to neuropathology research and education at Japanese medical schools. I have the impression that neuropathology is a subdivision of pathology, particularly when considering biopsy diagnosis of CNS tumors. However, it still appears to be difficult to find any faculty members who deal with neuropathology in pathology departments. In this sense, there is concern that our society membership will gradually decline, despite the old slogan that “the 21st century is the age of brain science” in Japan. I also served as Editor-in-Chief of our society journal Neuropathology (2003-2011). Although my memory is vague, when I accepted this position, the papers published in Neuropathology were already searchable on PubMed, and probably already had an established journal impact factor (IF). On my watch, the IF exceeded 2.0 once or twice (cf. IF 2021: 2.076). It was also a pleasure to receive manuscripts submitted from abroad. During my time, submissions from China and Korea showed an increasing trend. I do not mind the high number of case reports in the journal. If it serves the role of an international neuropathology journal, I am glad. After I invited Dr. Min-Cheol Lee to Niigata in 2007, I made several Korean friends who were pathologists at the University College of Medicine. On December 8, 2012, the “Seoul Neuropathology Forum” was held under the sponsorship of Seoul National University Hospital (Dr. Sung-Hye Park). Dr. Park is a self-proclaimed neuropathologist belonging to the Department of Pathology and one of the leaders of the Neuropathology Study Group of the Korean Society of Pathologists. They are experts in the pathological diagnosis of CNS tumors and allied diseases. I was very impressed by the Forum entitled “Neurodegenerative diseases – Up to date”. Their work confirmed that they were unmistakably neuropathologists (Fig. 18).
Figure 18: Seoul Neuropathology Forum in Seoul (December 8, 2012). Front row, left to right: Drs. Tetsuaki Arai (Tsukuba), Kazuhiko Watabe (Tokyo), Yeon-Lim Suh (Seoul), Shin Kwang Khang (Seoul), Yue-Shan Piao (Beijing), HT (Niigata), Min-Cheol Lee (Gwangju) and En Kyung Hong (Seoul). Top Row, left to right (except for one on the left and one on the right): Drs. Kyung-Wha Lee (Seoul), Jang-Hee Kim (Suwon), Narae Kim (Seongnam), Sung-Hye Park (Seoul), Se-Hoon Kim (Seoul), Ghee-Young Choe (Seoul) and Yeon-Soo Lee (Seoul). I succeeded Dr. Herbert Budka as President (2014-2018) of the International Society of Neuropathology (ISN). I do not remember the date exactly, but I received an e-mail message from Dr. Francesco Scaravilli saying that he was considering nominating me as President-elect of the ISN. I believe he had a role as a society officer of the ISN at that time. When I was in Dr. Suzuki’s lab in New York, I first became aware of his name because it was often on Dr. Kuni’s lips (later his and Kuni’s names appeared in Nature 305; 713-5, 1983). I felt a sense of intimacy with him, despite never having met him. Finally, I accepted his offer, and replied to his e-mail with a brief document introducing my career in research and teaching. However, I still do not know why he chose me. During my Presidency, one of my fond memories was going to Hyderabad, India with Dr. Budka, Dr. David W. Ellison and Dr. Raj Kalaria in December 2015 to celebrate the official establishment of the Neuropathology Society of India (NPSI) as well as the First Annual Conference of the NPSI (Fig.19). We had a good time with NPSI officers and participants, the latter including many young residents. I had a reunion with Dr. Chitra Sarkar, and had a chance to take a walk around the town with Dr. Budka, who said, “Hitoshi, beware of the dogs on the street”, to which I answered, “Certainly”.
Figure 19: Taking part in the 1st Annual Conference of the Neuropathology Society of India held in Hyderabad (December 2015). Left to right: Dr. David W. Ellison, HT, Dr. Raj Kalaria and Dr. Herbert Budka. We were the ISN delegation of four. Lastly, I would like to mention the Asian Oceanian Society of Neuropathology (AOSN), which was officially established as an offshoot of the Asian Society of Neuropathology (ASN) on September 25, 2018, at the 4th Asian Congress of Neuropathology held in conjunction with the 19th ICN in Tokyo (Fig. 20). I was very happy to have been involved in the establishment of the ASN (1st Congress in 2008 in Tokyo) from its inception (Asian Neuropathology Workshop in 2007 in Tokyo). I sincerely hope that the AOSN will continue to develop further in the future.
Figure 20: Asian Society of Neuropathology General Assembly in Tokyo (September 25, 2018). Members present. Front row, left to right: Drs. Glenda Halliday (Sydney), Mari Yoshida (Nagoya), Anita Mahadevan (Bangalore), Catriona A. McLean (Melbourne), Yue-Shan Piao (Beijing) and Vani Santosh (Bangalore). Top row, left to right: Drs. Ranil de Silva (Colombo), Tarik Tihan (San Francisco, as a representative of Turkey), Lai Siang Hui (Singapore), Ho-Keung Ng (Hong Kong), Shigeo Murayama (Tokyo), HT (Niigata), Takashi Komori (Tokyo), Bishan Dass Radotra (Chandigarh) and Thong K. Wong (Kuala Lumpur). Members absent. Dr. Sung-Hye Park (Seoul) and Dr. Maysa Ai-Hussaini (Amman). Thinking back to all these experiences, I must say that I really enjoyed my various roles with the kind help of many domestic and international colleagues. I have really enjoyed not only my work but also my interactions with my colleagues and friends. Retirement and Departure I retired from my faculty position at Niigata University at the age of 65 in late March 2018. In fact, I left my university at the end of January 2020, and I have spent the last 6 years, including the concurrent appointment as a professor for the first 4 years, as Executive Vice-President for Research at my alma mater (Fig. 21).
Figure 21: HT desk-working at his personal computer (November 7, 2016). At the invitation of my old friend, Dr. K. Onda (neurosurgeon; Director), I am currently working as Head of Laboratory Medicine and Head of Research at Niigata Neurosurgical Hospital, a major hospital in Niigata City specializing in cerebrovascular diseases, while maintaining a relationship with the Department of Pathology, BRI, as professor emeritus. I am still an active neuropathologist. Fortunately, my senior colleague Dr. Takeda also works at this Hospital as Head of Pathology. I have started studying the neuropathology of cerebrovascular diseases, which is an unfamiliar field to me. My teacher Dr. Ikuta passed away on May 26, 2021 at the age of 92. He was a pioneer of neuropathology in Japan and had many pupils who are distributed widely from Hokkaido in the north to Okinawa in the south. He had worked as Director of the Brain Research Center affiliated with this Hospital for a long period after his retirement (1995-2015). He told me that during his life he was very happy to have had so many colleagues and friends abroad. Most of them have passed away now. Time flies like an arrow. Enjoying life together Several months after my wife Shizue passed away, Dr. Ikuta told me that it might be difficult for me to fulfill my mission alone as a professor. After that, when I returned to my parents’ home, my mother told me that although I was not “fat”, I was swollen. I suddenly started to worry about my health. Some of my friends in my academic societies sent me e-mails, telling me to get married as soon as possible and that they would find a bride for me; I sent them my pictures right away. In the end, I remarried in June 2001 after being introduced to a lady named Yuriko by a friend. Dr. Ikuta often told me that Yuriko has made me what I am today. Although I am not good at expressing my gratitude, I almost always took her with me to academic conferences at home and abroad. On each occasion, she spent a pleasant time talking with my young fellows and my friends’ wives (Fig. 15). Unfortunately, we have no children. However, we have 4 female Chinese pupils, and Yuriko is always happy to see photos of the growing children sent via e-mail by three of them (Drs. Piao, Tan and Fu). She looks upon them as if they were her own grandchildren, and also has motherly concern about when the fourth pupil (Dr. Zhang) will get married. She is a trained pianist and her hobby is ikebana (flower arrangement). She is a master of Ikenobo ikebana and also a good tennis player. I do not have such talents. However, I enjoy self-produced greetings with ikebana that signal “I am home” and “welcome home” in the entrance hall. As to sports, I am still a football freak, although I no longer play. Since retirement, I have come to enjoy wandering in fields observing butterflies as a sort of intellectual curiosity. We both enjoy this together on weekends, and intend to continue appreciating life together as much as possible. We cannot wait for the COVID-19 pandemic to go away. Concluding remarks I genuinely appreciate the fact I was able to meet my two teachers, Dr. Ikuta and Dr. Suzuki, though I can’t be certain whether I met their expectations or not. I was not necessarily an expert in any particular field, such as neurodegenerative diseases, or any particular disease, such as ALS, and I had no strong intention of becoming one. I suppose my specialty would be neuropathology, specifically diagnostic neuropathology, whereby even with a diagnosis, hidden new features may be found and a new disease may emerge. I have no doubt that I have been a teacher, but also always a trainee. I am very pleased that I have been able to go through a series of epochs in neuropathology characterized by the use of electron microscopy, IHC and molecular genetics. I have many colleagues to thank for their friendship, which continues to the present day. Addendum During my tenure as a professor, I have genuinely enjoyed and practiced neuropathology with the faculty and staff, as well as residents and graduate students. I would like to leave a list of their names with gratitude. Mitsunori Yamada, Koichi Wakabayashi, Akiyoshi Kakita, Koichi Kawasaki, Shintaro Hayashi, Keisuke Iwanaga, Mu Su, Yasuko Hayashi (Toyoshima), Yue-Shan Piao, Chikanori Inenaga, Chun-Feng Tan, Tsutomu Sugai, Mari Tada, Kenji Sakai, Yasushi Nishihira, Koshun Matsuo, Masae Ryufuku, Misato Yamazaki, Hiroki Kitaura, Hiroshi Shimizu, Kenichi Okazaki, Ying-Jun Zheng, Yoshiko Sakuma, Ming-Wei Zhu, Yong-Juan Fu, Takayuki Kosaka, Yasuhiro Hoshi, Manabu Natsumeda, Yukari Miki, Hiroaki Miyahara, Kenichi Soma, Makiko Matsuda, Atsushi Shiga, Ryosuke Ogura, Yuichi Yokoyama, Ryoko Takeuchi, Tadashi Kimura, Hai-Shan Jiang, Hidetomo Tanaka, Naohiko Seike, Tomoe Sato, Rie Saito, Lu Zhang, Junko Ito, Akari Takeshima, Asa Nakahara and Takanori Nozawa. The staff who have worked prolonged periods: Shigekimi Egawa, Tomiyoshi Hasegawa, Yuko Ota, Chieko Tanda, Junko Takasaki and Shingo Nigorikawa (technical), and Mihoko Machida and Mari Yoshida (office).
Copyright: © 2023 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |